

Transient cerebral hypoperfusion and hypertensive events during atrial fibrillation: a plausible mechanism for cognitive impairment
- PMID: 27334559
- PMCID: PMC4917883
- DOI: 10.1038/srep28635
Transient cerebral hypoperfusion and hypertensive events during atrial fibrillation: a plausible mechanism for cognitive impairment
Abstract
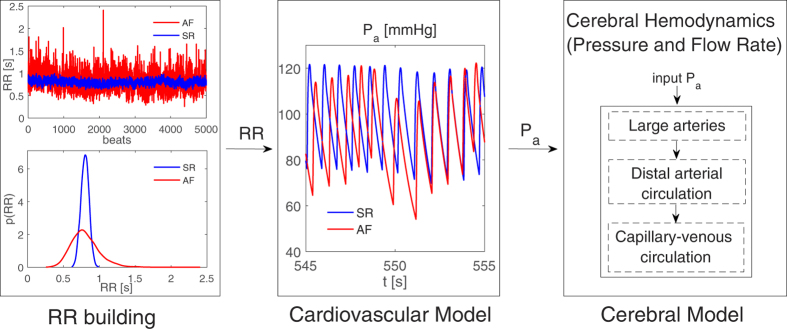
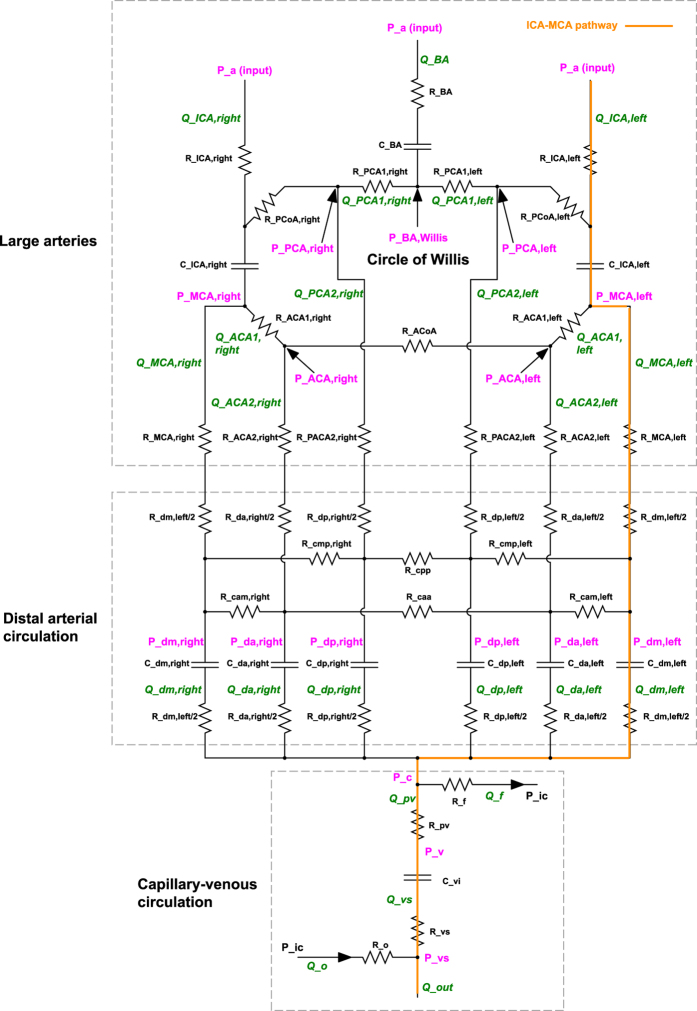
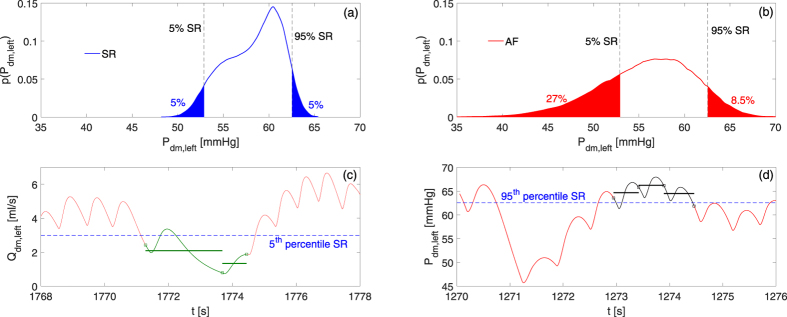
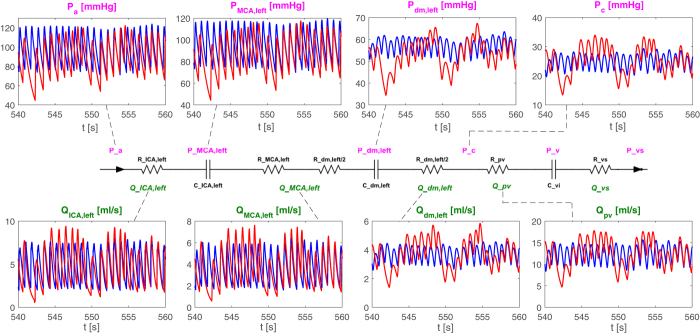
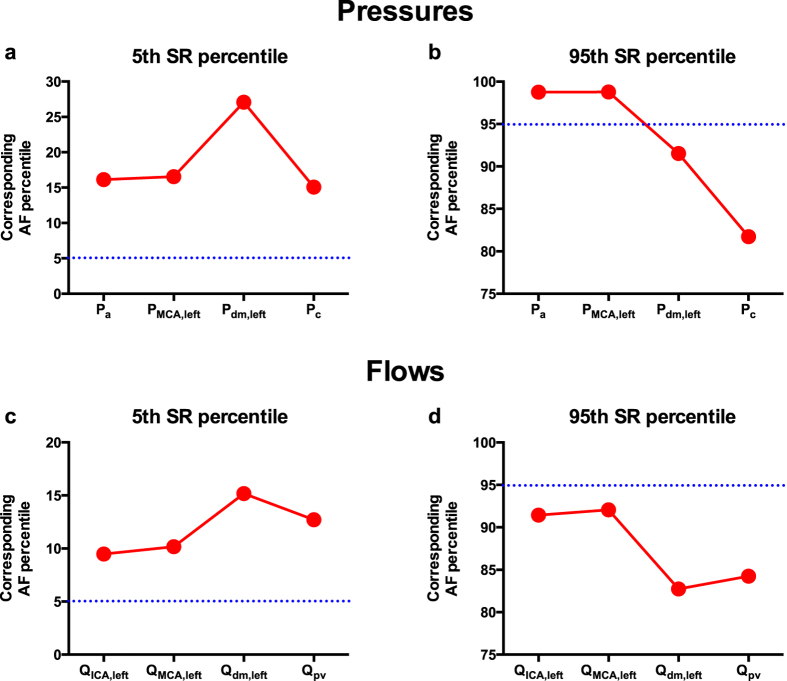
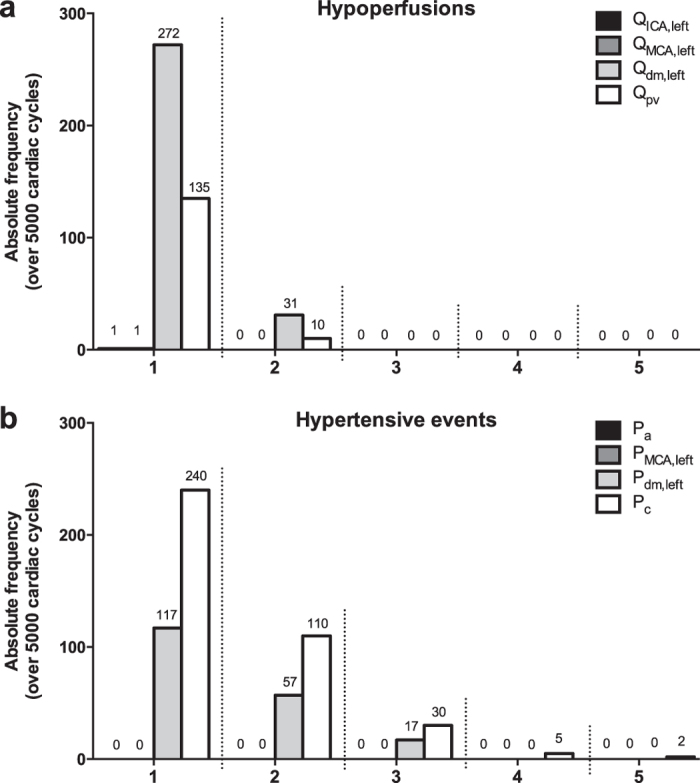
Atrial fibrillation (AF) is associated with an increased risk of dementia and cognitive decline, independent of strokes. Several mechanisms have been proposed to explain this association, but altered cerebral blood flow dynamics during AF has been poorly investigated: in particular, it is unknown how AF influences hemodynamic parameters of the distal cerebral circulation, at the arteriolar and capillary level. Two coupled lumped-parameter models (systemic and cerebrovascular circulations, respectively) were here used to simulate sinus rhythm (SR) and AF. For each simulation 5000 cardiac cycles were analyzed and cerebral hemodynamic parameters were calculated. With respect to SR, AF triggered a higher variability of the cerebral hemodynamic variables which increases proceeding towards the distal circulation, reaching the maximum extent at the arteriolar and capillary levels. This variability led to critical cerebral hemodynamic events of excessive pressure or reduced blood flow: 303 hypoperfusions occurred at the arteriolar level, while 387 hypertensive events occurred at the capillary level during AF. By contrast, neither hypoperfusions nor hypertensive events occurred during SR. Thus, the impact of AF per se on cerebral hemodynamics candidates as a relevant mechanism into the genesis of AF-related cognitive impairment/dementia.
Figures
Similar articles
-
Higher ventricular rate during atrial fibrillation relates to increased cerebral hypoperfusions and hypertensive events.Sci Rep. 2019 Mar 7;9(1):3779. doi: 10.1038/s41598-019-40445-5. Sci Rep. 2019. PMID: 30846776 Free PMC article.
-
Alteration of cerebrovascular haemodynamic patterns due to atrial fibrillation: an in silico investigation.J R Soc Interface. 2017 Apr;14(129):20170180. doi: 10.1098/rsif.2017.0180. J R Soc Interface. 2017. PMID: 28446702 Free PMC article.
-
Investigating the impact of atrial fibrillation on the vascular onset of glaucoma via multiscale cardiovascular modeling.Comput Methods Programs Biomed. 2025 Jul;267:108783. doi: 10.1016/j.cmpb.2025.108783. Epub 2025 Apr 22. Comput Methods Programs Biomed. 2025. PMID: 40286418
-
Mechanisms, Clinical Significance, and Prevention of Cognitive Impairment in Patients With Atrial Fibrillation.Can J Cardiol. 2017 Dec;33(12):1556-1564. doi: 10.1016/j.cjca.2017.09.024. Epub 2017 Oct 6. Can J Cardiol. 2017. PMID: 29173598 Review.
-
The role of atrial fibrillation in vascular cognitive impairment and dementia: epidemiology, pathophysiology, and preventive strategies.Geroscience. 2025 Feb;47(1):287-300. doi: 10.1007/s11357-024-01290-1. Epub 2024 Aug 13. Geroscience. 2025. PMID: 39138793 Free PMC article. Review.
Cited by
-
Insights from computational modeling on the potential hemodynamic effects of sinus rhythm versus atrial fibrillation.Front Cardiovasc Med. 2022 Sep 14;9:844275. doi: 10.3389/fcvm.2022.844275. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36187015 Free PMC article. Review.
-
Cerebral hemodynamics during atrial fibrillation: Computational fluid dynamics analysis of lenticulostriate arteries using 7 T high-resolution magnetic resonance imaging.Phys Fluids (1994). 2022 Dec;34(12):121909. doi: 10.1063/5.0129899. Epub 2022 Dec 29. Phys Fluids (1994). 2022. PMID: 36776539 Free PMC article.
-
Atrial fibrillation hemodynamic effects on lenticulostriate arteries identified at 7-Tesla cerebral magnetic resonance imaging.Clin Transl Med. 2023 Sep;13(9):e1367. doi: 10.1002/ctm2.1367. Clin Transl Med. 2023. PMID: 37735820 Free PMC article. No abstract available.
-
Association between Blood Pressure, Blood Pressure Variability, and Post-Stroke Cognitive Impairment.Biomedicines. 2021 Jul 2;9(7):773. doi: 10.3390/biomedicines9070773. Biomedicines. 2021. PMID: 34356837 Free PMC article. Review.
-
Heart-brain interaction in cardiogenic dementia: pathophysiology and therapeutic potential.Front Cardiovasc Med. 2024 Jan 24;11:1304864. doi: 10.3389/fcvm.2024.1304864. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38327496 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
