

Burden of emergency conditions and emergency care usage: new estimates from 40 countries
- PMID: 27334758
- PMCID: PMC5179323
- DOI: 10.1136/emermed-2016-205709
Burden of emergency conditions and emergency care usage: new estimates from 40 countries
Abstract
Objective: To estimate the global and national burden of emergency conditions, and compare them to emergency care usage rates.
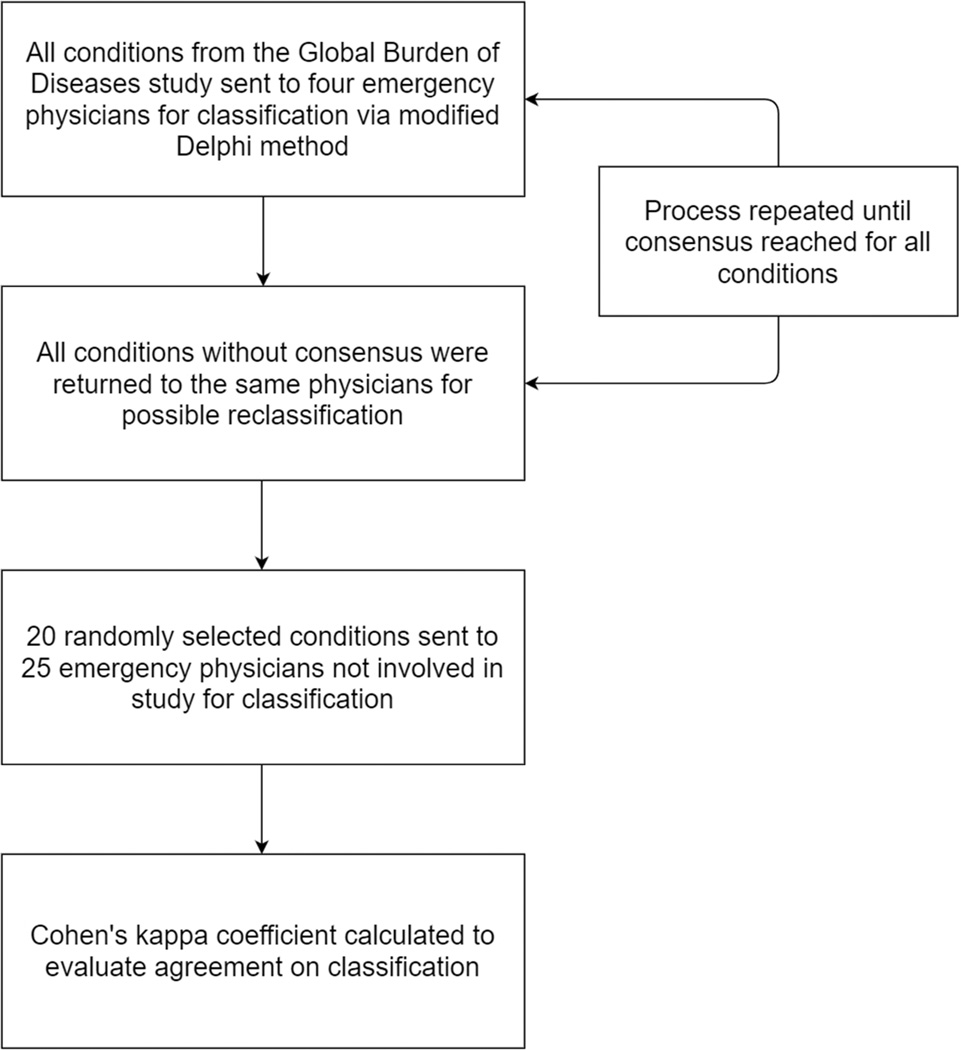
Methods: We coded all 291 Global Burden of Disease 2010 conditions into three categories to estimate emergency burden: conditions that, if not addressed within hours to days of onset, commonly lead to serious disability or death; conditions with common acute decompensations that lead to serious disability or death; and non-emergencies. Emergency care usage rates were obtained from a systematic literature review on emergency care facilities in low-income and middle-income countries (LMICs), supplemented by national health system reports.
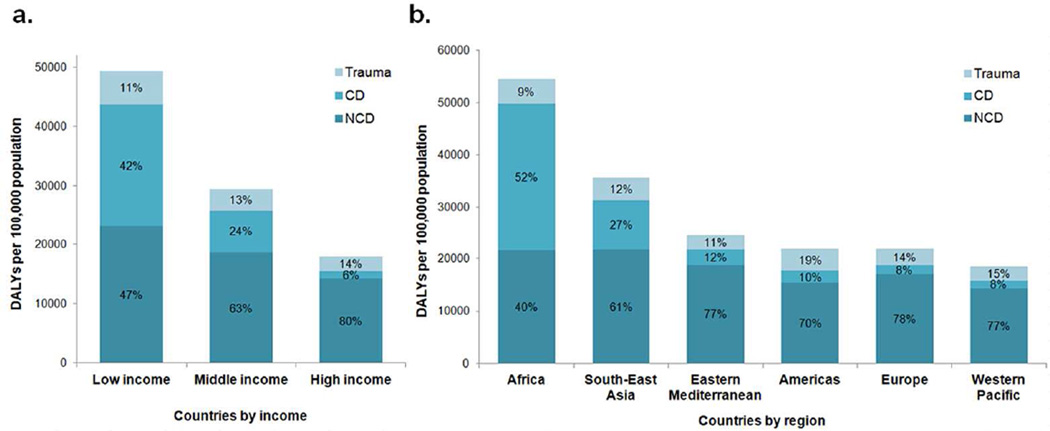
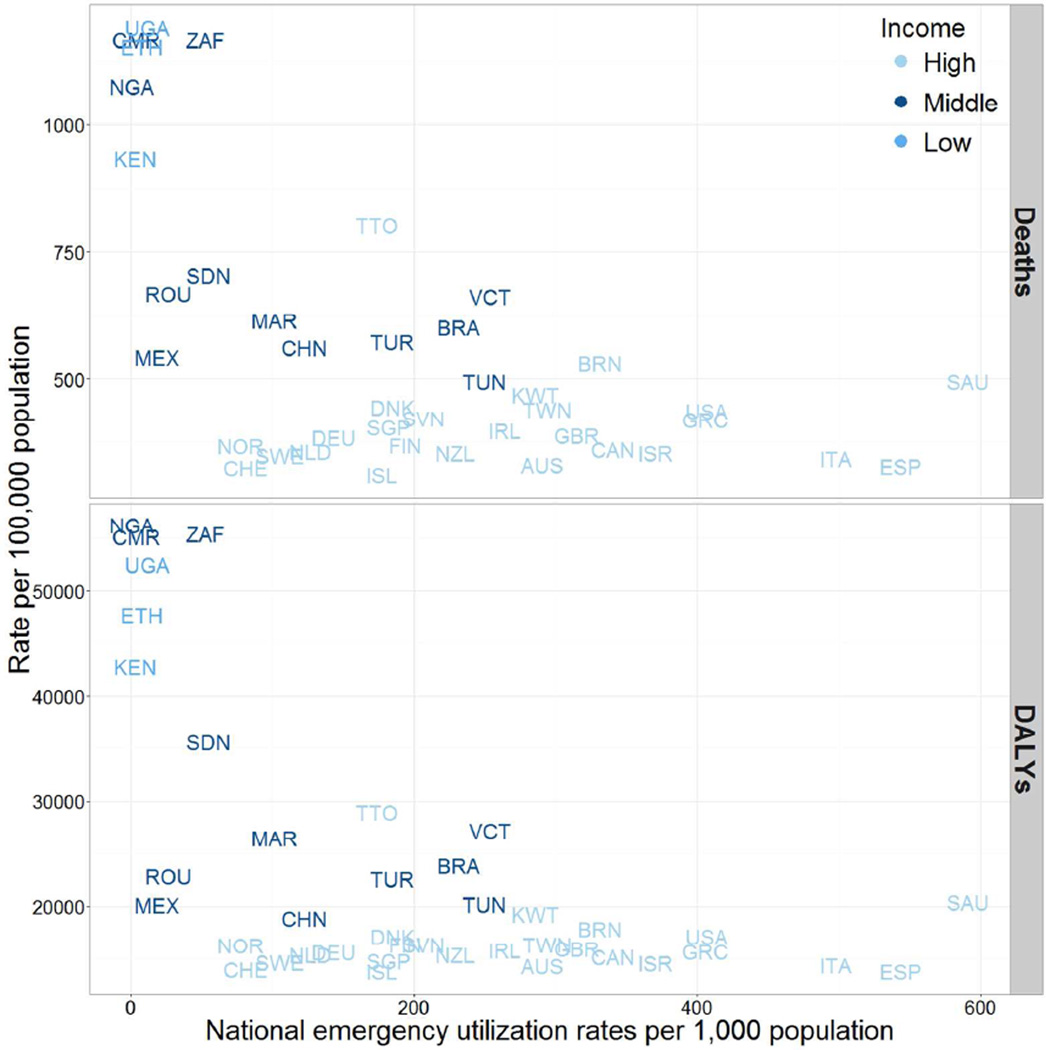
Findings: All 15 leading causes of death and disability-adjusted life years (DALYs) globally were conditions with potential emergent manifestations. We identified 41 facility-based reports in 23 countries, 12 of which were in LMICs; data for 17 additional countries were obtained from national or regional reports on emergency usage. Burden of emergency conditions was the highest in low-income countries, with median DALYs of 47 728 per 100 000 population (IQR 45 253-50 085) in low-income, 25 186 (IQR 21 982-40 480) in middle-income and 15 691 (IQR 14 649-16 382) in high-income countries. Patterns were similar using deaths to measure burden and excluding acute decompensations from the definition of emergency conditions. Conversely, emergency usage rates were the lowest in low-income countries, with median 8 visits per 1000 population (IQR 6-10), 78 (IQR 25-197) in middle-income and 264 (IQR 177-341) in high-income countries.
Conclusions: Despite higher burden of emergency conditions, emergency usage rates are substantially lower in LMICs, likely due to limited access to emergency care.
Keywords: access to care; emergency care systems; emergency department utilisation; global health.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Figures
References
-
- Anderson PD, Suter RE, Mulligan T, et al. World Health Assembly Resolution 60.22 and Its Importance as a Health Care Policy Tool for Improving Emergency Care Access and Availability Globally. Ann Emerg Med. 2012;60 35-44.e3. - PubMed
-
- Hsia R, Razzak J, Tsai AC, et al. Placing emergency care on the global agenda. Ann Emerg Med. 2010;56:142–149. - PubMed
-
- Calvello E, Reynolds T, Hirshon JM, et al. Emergency care in sub-Saharan Africa: Results of a consensus conference. Afr J Emerg Med. 2013;3:42–48.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical