

Enhanced Islet Cell Nucleomegaly Defines Diffuse Congenital Hyperinsulinism in Infancy but Not Other Forms of the Disease
- PMID: 27334808
- PMCID: PMC4922485
- DOI: 10.1093/ajcp/aqw075
Enhanced Islet Cell Nucleomegaly Defines Diffuse Congenital Hyperinsulinism in Infancy but Not Other Forms of the Disease
Abstract
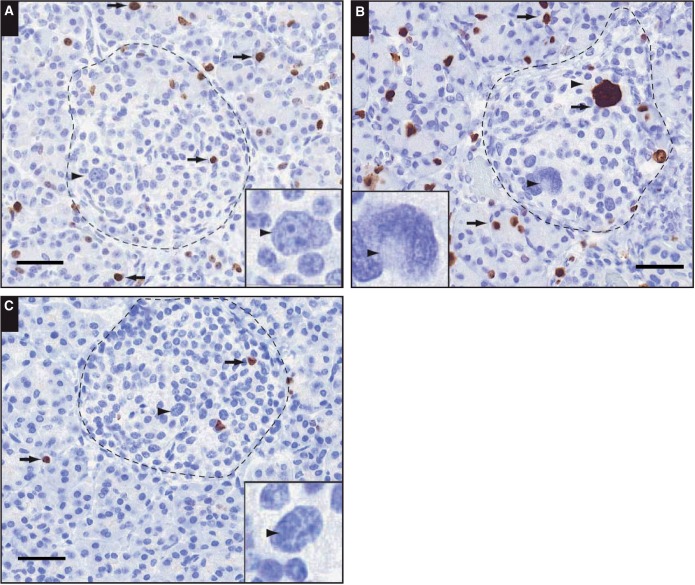
Objectives: To quantify islet cell nucleomegaly in controls and tissues obtained from patients with congenital hyperinsulinism in infancy (CHI) and to examine the association of nucleomegaly with proliferation.
Methods: High-content analysis of histologic sections and serial block-face scanning electron microscopy were used to quantify nucleomegaly.
Results: Enlarged islet cell nuclear areas were 4.3-fold larger than unaffected nuclei, and the mean nuclear volume increased to approximately threefold. Nucleomegaly was a normal feature of pediatric islets and detected in the normal regions of the pancreas from patients with focal CHI. The incidence of nucleomegaly was highest in diffuse CHI (CHI-D), with more than 45% of islets containing two or more affected cells. While in CHI-D nucleomegaly was negatively correlated with cell proliferation, in all other cases, there was a positive correlation.
Conclusions: Increased incidence of nucleomegaly is pathognomonic for CHI-D, but these cells are nonproliferative, suggesting a novel role in the pathobiology of this condition.
Keywords: Congenital hyperinsulinism; Hyperplasia; Hypoglycemia; Insulin; Islet; Nucleomegaly; Pancreas; Serial block-face scanning electron microscopy; β cell.
© American Society for Clinical Pathology, 2016.
Figures







References
-
- Dunne MJ, Cosgrove KE, Shepherd RM, et al. Hyperinsulinism in infancy: from basic science to clinical disease. Physiol Rev. 2004;84:239-275. - PubMed
-
- Arya VB, Mohammed Z, Blankenstein O, et al. Hyperinsulinaemic hypoglycaemia. Horm Metab Res. 2014;46:157-170. - PubMed
-
- De Leon DD, Stanley CA. Mechanisms of disease: advances in diagnosis and treatment of hyperinsulinism in neonates. Nat Clin Pract Endocrinol Metab. 2007;3:57-68. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
