

Ultrafiltration Rates and the Quality Incentive Program: Proposed Measure Definitions and Their Potential Dialysis Facility Implications
- PMID: 27335126
- PMCID: PMC4974895
- DOI: 10.2215/CJN.13441215
Ultrafiltration Rates and the Quality Incentive Program: Proposed Measure Definitions and Their Potential Dialysis Facility Implications
Abstract
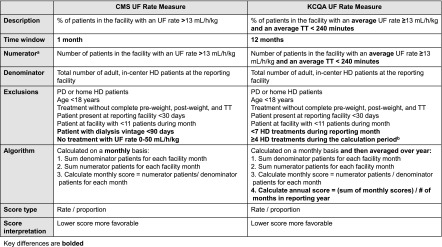
Background and objectives: Rapid ultrafiltration rates are associated with adverse outcomes among patients on hemodialysis. The Centers for Medicare and Medicaid Services is considering an ultrafiltration rate quality measure for the ESRD Quality Incentive Program. Two measure developers proposed ultrafiltration rate measures with different selection criteria and specifications. We aimed to compare the proposed ultrafiltration rate measures and quantify dialysis facility operational burden if treatment times were extended to lower ultrafiltration rates.
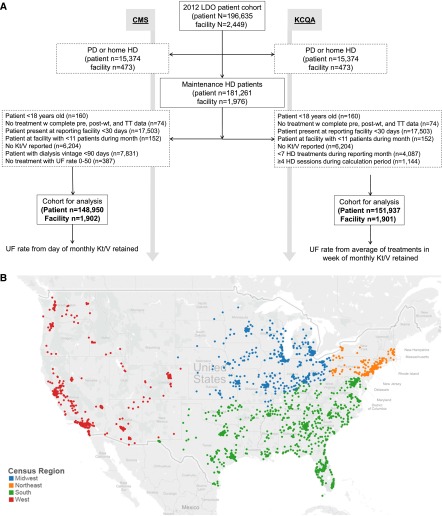
Design, setting, participants, & measurements: Data were taken from the 2012 database of a large dialysis organization. Analyses of the Centers for Medicare and Medicaid Services measure considered 148,950 patients on hemodialysis, and analyses of the Kidney Care Quality Alliance measure considered 151,937 patients. We described monthly patient and facility ultrafiltration rates and examined differences in patient characteristics across ultrafiltration rate thresholds and differences in facilities across ultrafiltration rate measure scores. We computed the additional treatment time required to lower ultrafiltration rates <13 ml/h per kilogram.
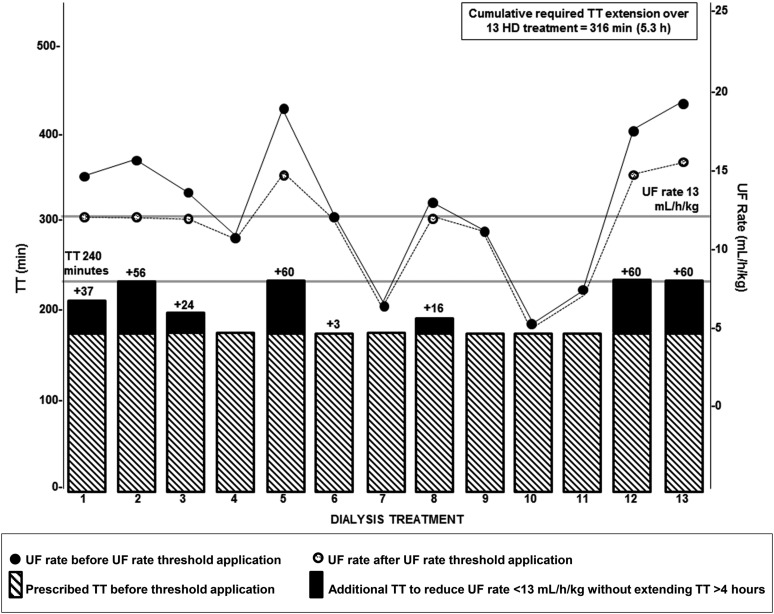
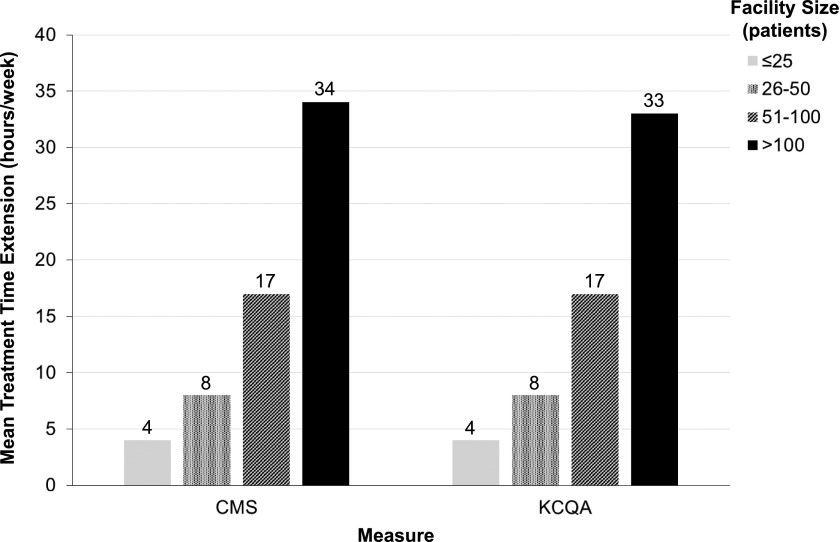
Results: Ultrafiltration rates peaked in winter and nadired in summer. Patients with higher ultrafiltration rates were younger; more likely to be women, nonblack, Hispanic, and lighter in weight; and more likely to have histories of heart failure compared with patients with lower ultrafiltration rates. Facilities had, on average, 20.8%±10.3% (July) to 22.8%±10.6% (February) of patients with ultrafiltration rates >13 ml/h per kilogram by the Centers for Medicare and Medicaid Services monthly measure. Facilities had, on average, 15.8%±8.2% of patients with ultrafiltration rates ≥13 ml/h per kilogram by the Kidney Care Quality Alliance annual measure. Larger facilities (>100 patients) would require, on average, 33 additional treatment hours per week to lower all facility ultrafiltration rates <13 ml/h per kilogram when total treatment time is capped at 4 hours.
Conclusions: Ultrafiltration rates vary seasonally and across clinical subgroups. Extension of treatment time as a strategy to lower ultrafiltration rates may pose facility operational challenges. Prospective studies of ultrafiltration rate threshold implementation are needed.
Keywords: Epidemiology and outcomes; Humans; Kidney Failure, Chronic; Medicaid; Medicare; Prospective Studies; heart failure; hemodialysis; renal dialysis; ultrafiltration.
Copyright © 2016 by the American Society of Nephrology.
Figures
Comment in
-
Fluid First or Not So Fast: Ultrafiltration Rate and the ESRD Quality Incentive Program.Clin J Am Soc Nephrol. 2016 Aug 8;11(8):1330-1332. doi: 10.2215/CJN.05840616. Epub 2016 Jun 22. Clin J Am Soc Nephrol. 2016. PMID: 27335125 Free PMC article. No abstract available.
References
-
- Weiner DE, Brunelli SM, Hunt A, Schiller B, Glassock R, Maddux FW, Johnson D, Parker T, Nissenson A: Improving clinical outcomes among hemodialysis patients: A proposal for a “volume first” approach from the chief medical officers of US dialysis providers. Am J Kidney Dis 64: 685–695, 2014 - PubMed
-
- Agar JW: Personal viewpoint: Limiting maximum ultrafiltration rate as a potential new measure of dialysis adequacy. Hemodial Int 20: 15–21, 2016 - PubMed
-
- National Quality Forum: About us. Available at: http://www.qualityforum.org/story/About_Us.aspx. Accessed November 30, 2015
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
