

Time-dependent changes in mortality and transformation risk in MDS
- PMID: 27335276
- PMCID: PMC5161006
- DOI: 10.1182/blood-2016-02-700054
Time-dependent changes in mortality and transformation risk in MDS
Abstract
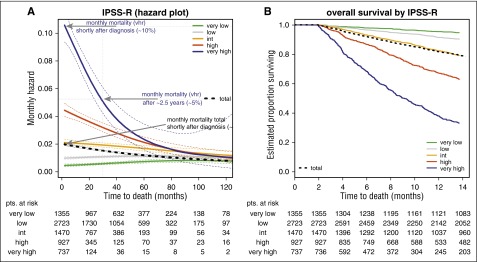
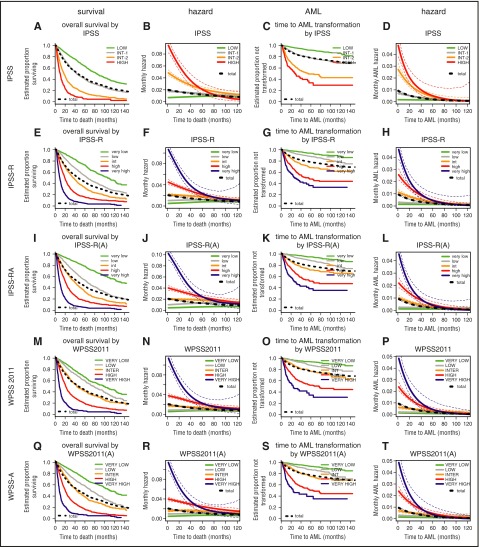
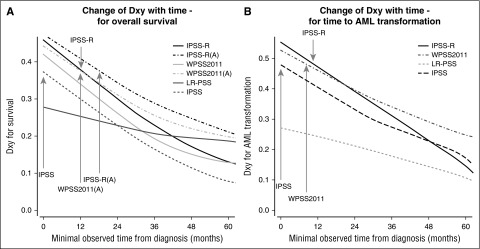
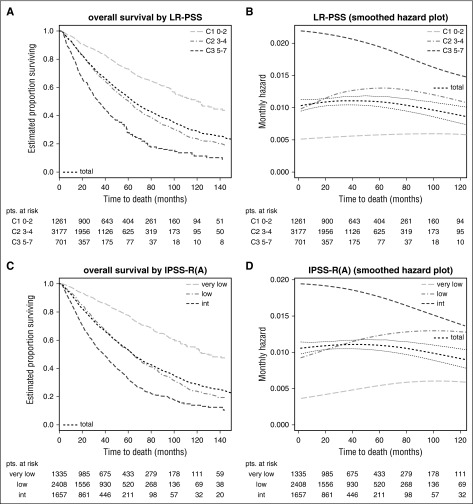
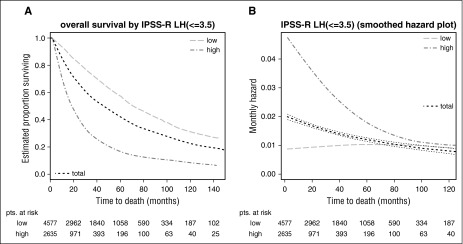
In myelodysplastic syndromes (MDSs), the evolution of risk for disease progression or death has not been systematically investigated despite being crucial for correct interpretation of prognostic risk scores. In a multicenter retrospective study, we described changes in risk over time, the consequences for basal prognostic scores, and their potential clinical implications. Major MDS prognostic risk scoring systems and their constituent individual predictors were analyzed in 7212 primary untreated MDS patients from the International Working Group for Prognosis in MDS database. Changes in risk of mortality and of leukemic transformation over time from diagnosis were described. Hazards regarding mortality and acute myeloid leukemia transformation diminished over time from diagnosis in higher-risk MDS patients, whereas they remained stable in lower-risk patients. After approximately 3.5 years, hazards in the separate risk groups became similar and were essentially equivalent after 5 years. This fact led to loss of prognostic power of different scoring systems considered, which was more pronounced for survival. Inclusion of age resulted in increased initial prognostic power for survival and less attenuation in hazards. If needed for practicability in clinical management, the differing development of risks suggested a reasonable division into lower- and higher-risk MDS based on the IPSS-R at a cutoff of 3.5 points. Our data regarding time-dependent performance of prognostic scores reflect the disparate change of risks in MDS subpopulations. Lower-risk patients at diagnosis remain lower risk whereas initially high-risk patients demonstrate decreasing risk over time. This change of risk should be considered in clinical decision making.
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Defining risk in MDS over time.Blood. 2016 Aug 18;128(7):885-6. doi: 10.1182/blood-2016-07-724930. Blood. 2016. PMID: 27539994 No abstract available.
References
-
- Adès L, Itzykson R, Fenaux P. Myelodysplastic syndromes. Lancet. 2014;383(9936):2239–2252. - PubMed
-
- Pfeilstöcker M. Prognostic Scoring in MDS. In: Varkonyi J, editor. The Myelodysplastic Syndromes. Dordrecht, The Netherlands: Springer; 2011. pp. 103–120.
-
- Pfeilstöcker M, Tüchler H, Schönmetzler A, Nösslinger T, Pittermann E. Time changes in predictive power of established and recently proposed clinical, cytogenetical and comorbidity scores for Myelodysplastic Syndromes. Leuk Res. 2012;36(2):132–139. - PubMed
-
- Malcovati L, Germing U, Kuendgen A, et al. Time-dependent prognostic scoring system for predicting survival and leukemic evolution in myelodysplastic syndromes. J Clin Oncol. 2007;25(23):3503–3510. - PubMed
-
- Garcia-Manero G, Shan J, Faderl S, et al. A prognostic score for patients with lower risk myelodysplastic syndrome. Leukemia. 2008;22(3):538–543. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
