

Retrospective Review of Current Nasojejunal Tube Insertion Practice
- PMID: 27335939
- PMCID: PMC4784621
- DOI: 10.1177/2333794X14568453
Retrospective Review of Current Nasojejunal Tube Insertion Practice
Abstract
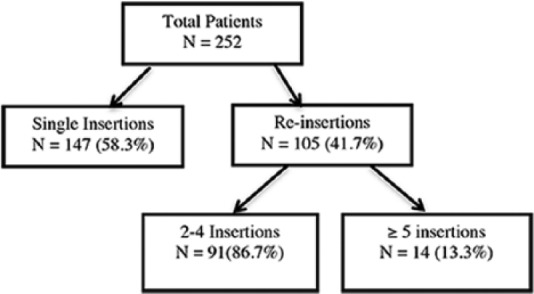
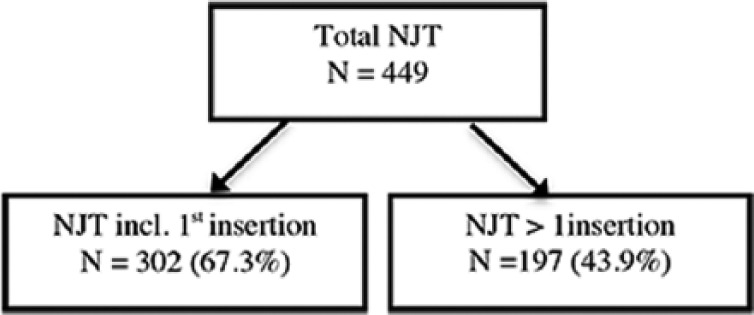
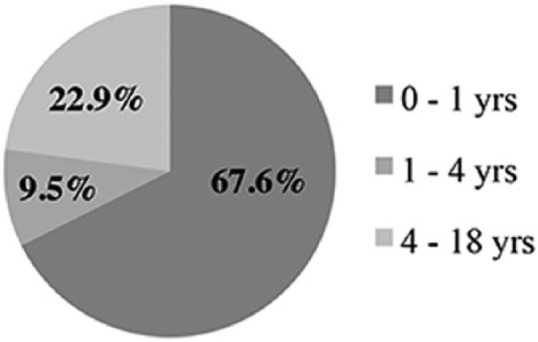
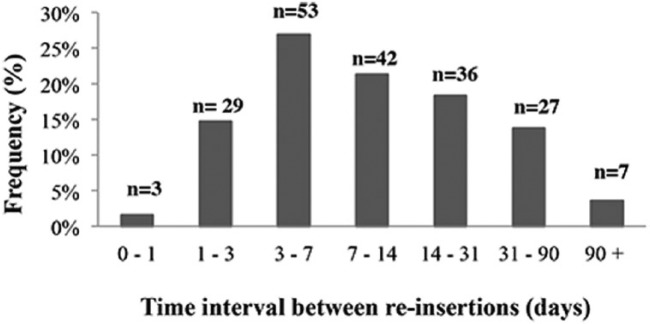
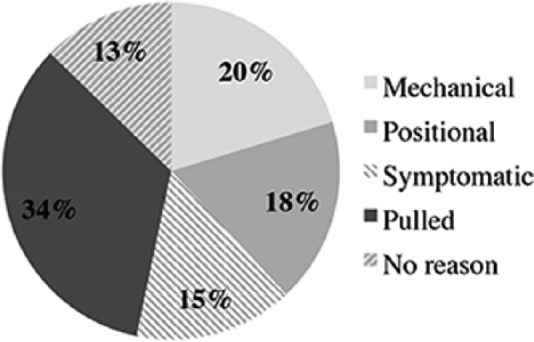
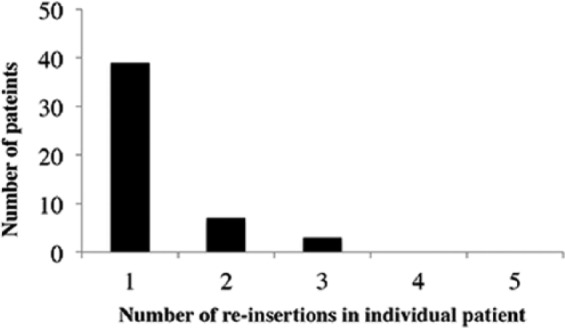
Repeated fluoroscopically guided nasojejunal tube (NJT) insertions, particularly in children, can pose health risks through increased radiation exposure. We analyzed frequency of NJT reinsertions and associated radiation exposure through retrospective evaluation of children <18 years at our institution who underwent fluoroscopically guided NJT insertions from 2007 to 2012. Age and weight, reinsertion frequency per patient, radiation dose (dose actual percentage [DAP]), time interval between, and indication for reinsertion were recorded. A total of 252 children (3 days to17 years, 11 months) had 449 NJT insertions. Reinsertions occurred in 105 (41.7%) patients with 14 (5.6%) having ≥5 reinsertions, and 67.6% of reinsertions occurring in patients <1 year. Mean DAP increased with frequency of reinsertion, along with age and weight. Most common indication for reinsertion was a pulled NJT (34.0%). Fluoroscopic NJT reinsertion was most frequent in younger, smaller patients. Self-guided, bedside NJT insertion, and/or earlier instigation of definitive nutritional therapy delivery should be considered.
Keywords: children; fluoroscopy; nasojejunal tube; radiation dose; self-guided technique.
Conflict of interest statement
Figures
Similar articles
-
Examination of the effectiveness of bedside nasojejunal tube placement using a portable imaging device with a flat panel detector.Nagoya J Med Sci. 2022 Nov;84(4):772-781. doi: 10.18999/nagjms.84.4.772. Nagoya J Med Sci. 2022. PMID: 36544604 Free PMC article.
-
Fluoroscopy-guided insertion of nasojejunal tubes in children - setting local diagnostic reference levels.Pediatr Radiol. 2009 Nov;39(11):1203-8. doi: 10.1007/s00247-009-1362-y. Epub 2009 Sep 30. Pediatr Radiol. 2009. PMID: 19789863 Clinical Trial.
-
Evaluation of a new technique for endoscopic nasojejunal feeding-tube placement.Gastrointest Endosc. 2006 Apr;63(4):590-5. doi: 10.1016/j.gie.2005.10.043. Gastrointest Endosc. 2006. PMID: 16564857
-
Endoscopic- versus x-ray-guidance for placement of nasojejunal tubes in critically ill patients: a systematic review and meta-analysis of randomized controlled trials.Am J Transl Res. 2022 Apr 15;14(4):2134-2146. eCollection 2022. Am J Transl Res. 2022. PMID: 35559401 Free PMC article. Review.
-
Measuring and monitoring radiation dose during fluoroscopically guided procedures.Tech Vasc Interv Radiol. 2010 Sep;13(3):188-93. doi: 10.1053/j.tvir.2010.03.009. Tech Vasc Interv Radiol. 2010. PMID: 20723835 Review.
Cited by
-
Small Bowel Intussusception due to Nasojejunal Tube Placement in Neonates: A Case Report.Surg Case Rep. 2025;11(1):25-0228. doi: 10.70352/scrj.cr.25-0228. Epub 2025 Jul 19. Surg Case Rep. 2025. PMID: 40697279 Free PMC article.
References
LinkOut - more resources
Full Text Sources
