

Early interventions in risk groups for schizophrenia: what are we waiting for?
- PMID: 27336054
- PMCID: PMC4849435
- DOI: 10.1038/npjschz.2016.3
Early interventions in risk groups for schizophrenia: what are we waiting for?
Abstract
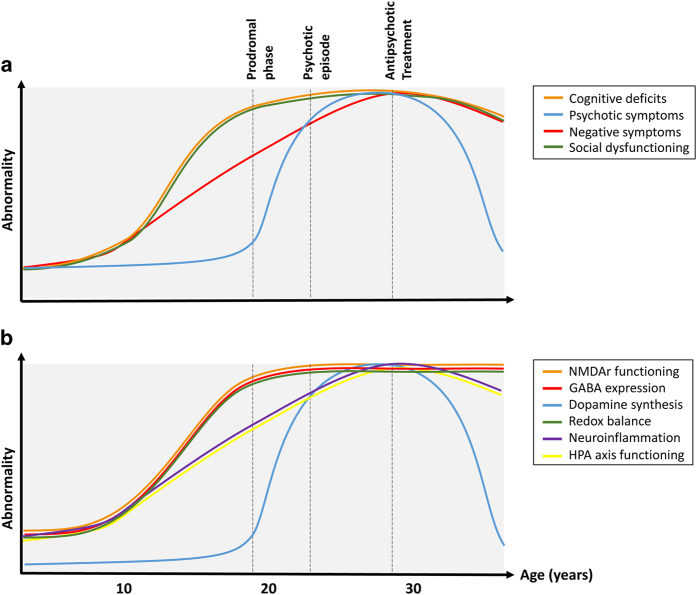
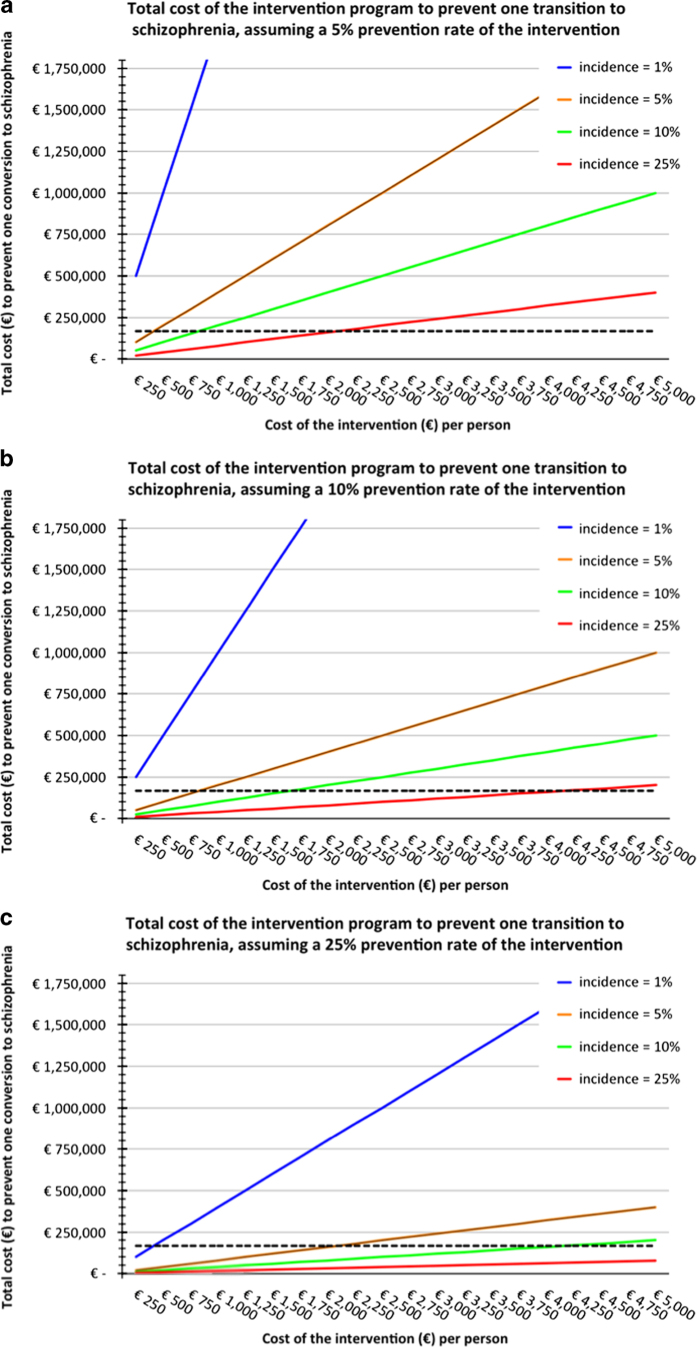
Intervention strategies in adolescents at ultra high-risk (UHR) for psychosis are promising for reducing conversion to overt illness, but have only limited impact on functional outcome. Recent studies suggest that cognition does not further decline during the UHR stage. As social and cognitive impairments typically develop before the first psychotic episode and even years before the UHR stage, prevention should also start much earlier in the groups at risk for schizophrenia and other psychiatric disorders. Early intervention strategies could aim to improve stress resilience, optimize brain maturation, and prevent or alleviate adverse environmental circumstances. These strategies should urgently be tested for efficacy: the prevalence of ~1% implies that yearly ~22 in every 100,000 people develop overt symptoms of this illness, despite the fact that for many of them-e.g., children with an affected first-degree family member or carriers of specific genetic variants-increased risk was already identifiable early in life. Our current ability to recognize several risk groups at an early age not only provides an opportunity, but also implies a clinical imperative to act. Time is pressing to investigate preventive interventions in high-risk children to mitigate or prevent the development of schizophrenia and related psychiatric disorders.
Figures
Similar articles
-
[Detection and early treatment of subjects at high risk of clinical psychosis: Definitions and recommendations].Encephale. 2017 May;43(3):292-297. doi: 10.1016/j.encep.2017.01.005. Epub 2017 Mar 25. Encephale. 2017. PMID: 28347521 Review. French.
-
[What support of young presenting a first psychotic episode, when schooling is being challenged?].Encephale. 2017 Dec;43(6):570-576. doi: 10.1016/j.encep.2017.10.001. Epub 2017 Nov 8. Encephale. 2017. PMID: 29128195 Review. French.
-
Early psychotic experiences: Interventions, problems and perspectives.Psychiatriki. 2015 Jan-Mar;26(1):45-54. Psychiatriki. 2015. PMID: 25880383 Review.
-
[Stress and psychotic transition: A literature review].Encephale. 2016 Aug;42(4):367-73. doi: 10.1016/j.encep.2015.10.001. Epub 2016 May 6. Encephale. 2016. PMID: 27161263 Review. French.
-
Attenuated psychotic and basic symptom characteristics in adolescents with ultra-high risk criteria for psychosis, other non-psychotic psychiatric disorders and early-onset psychosis.Eur Child Adolesc Psychiatry. 2016 Oct;25(10):1091-102. doi: 10.1007/s00787-016-0832-7. Epub 2016 Feb 26. Eur Child Adolesc Psychiatry. 2016. PMID: 26921232
Cited by
-
Self-reported sleep disturbances associated with procedural learning impairment in adolescents at ultra-high risk for psychosis.Schizophr Res. 2017 Dec;190:160-163. doi: 10.1016/j.schres.2017.03.025. Epub 2017 Mar 16. Schizophr Res. 2017. PMID: 28318840 Free PMC article.
-
30 Years on: How the Neurodevelopmental Hypothesis of Schizophrenia Morphed Into the Developmental Risk Factor Model of Psychosis.Schizophr Bull. 2017 Oct 21;43(6):1190-1196. doi: 10.1093/schbul/sbx121. Schizophr Bull. 2017. PMID: 28981842 Free PMC article.
-
Hippocampal Hyperactivity as a Druggable Circuit-Level Origin of Aberrant Salience in Schizophrenia.Front Pharmacol. 2020 Oct 16;11:486811. doi: 10.3389/fphar.2020.486811. eCollection 2020. Front Pharmacol. 2020. PMID: 33178010 Free PMC article. Review.
-
Developmental profiles of schizotypy in the general population: A record linkage study of Australian children aged 11-12 years.Br J Clin Psychol. 2022 Sep;61(3):836-858. doi: 10.1111/bjc.12363. Epub 2022 Mar 1. Br J Clin Psychol. 2022. PMID: 35229307 Free PMC article.
-
Blonanserin versus haloperidol in Japanese patients with schizophrenia: A phase 3, 8-week, double-blind, multicenter, randomized controlled study.Neuropsychopharmacol Rep. 2019 Sep;39(3):173-182. doi: 10.1002/npr2.12057. Epub 2019 Apr 30. Neuropsychopharmacol Rep. 2019. PMID: 31041855 Free PMC article. Clinical Trial.
References
-
- McGrath, J. , Saha, S. , Chant, D. & Welham, J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol. Rev. 30, 67–76 (2008). - PubMed
-
- Gustavsson, A. et al. Cost of disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 21, 718–779 (2011). - PubMed
-
- Harvey, P. D. Disability in schizophrenia: contributing factors and validated assessments. J. Clin. Psychiatry 75 Suppl 1, 15–20 (2014). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
