

Corticosteroid Use and Complications in a US Inflammatory Bowel Disease Cohort
- PMID: 27336296
- PMCID: PMC4918923
- DOI: 10.1371/journal.pone.0158017
Corticosteroid Use and Complications in a US Inflammatory Bowel Disease Cohort
Erratum in
-
Correction: Corticosteroid Use and Complications in a US Inflammatory Bowel Disease Cohort.PLoS One. 2018 May 9;13(5):e0197341. doi: 10.1371/journal.pone.0197341. eCollection 2018. PLoS One. 2018. PMID: 29742165 Free PMC article.
Abstract
Background and aims: Corticosteroids are effective for the short-term treatment of inflammatory bowel disease (IBD). Long-term use, however, is associated with significant adverse effects. To define the: (1) frequency and duration of corticosteroid use, (2) frequency of escalation to corticosteroid-sparing therapy, (3) rate of complications related to corticosteroid use, (4) rate of appropriate bone density measurements (dual energy X-ray absorptiometry [DEXA] scans), and (5) factors associated with escalation and DEXA scans.
Methods: Retrospective review of Veterans Health Administration (VHA) data from 2002-2010.
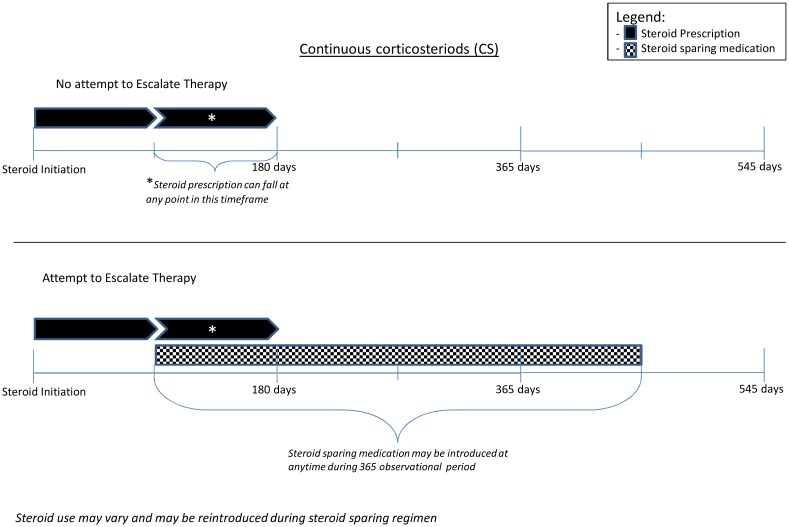
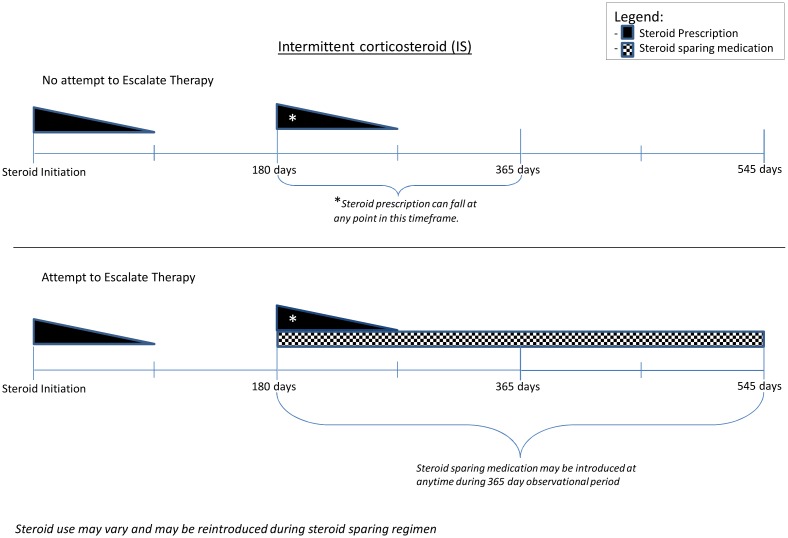
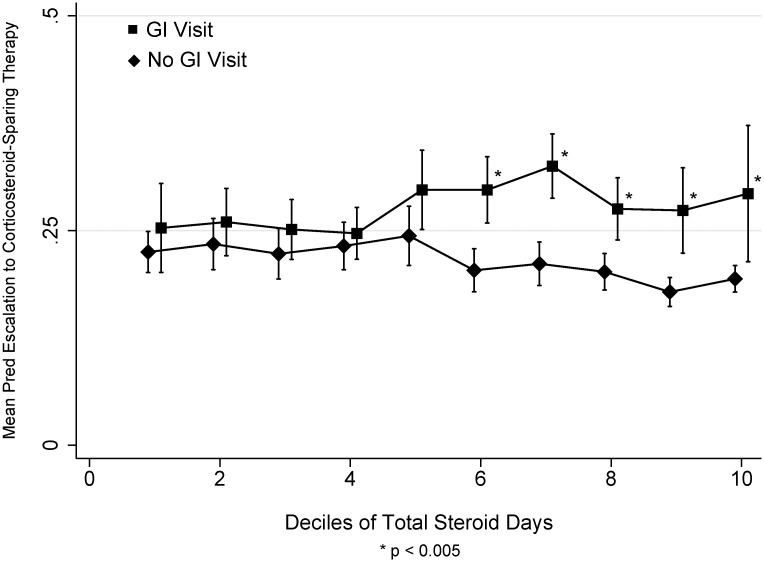
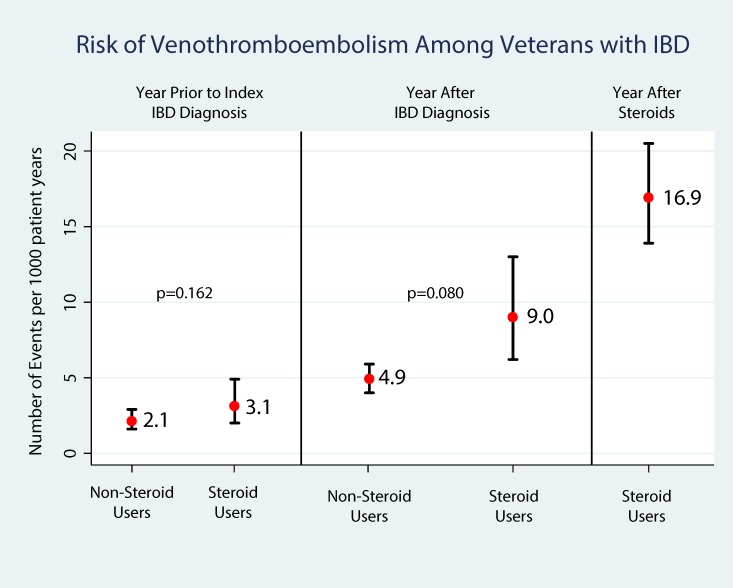
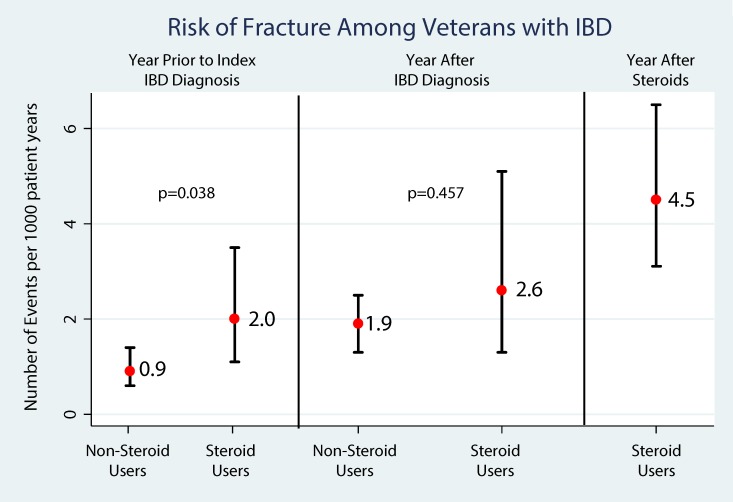
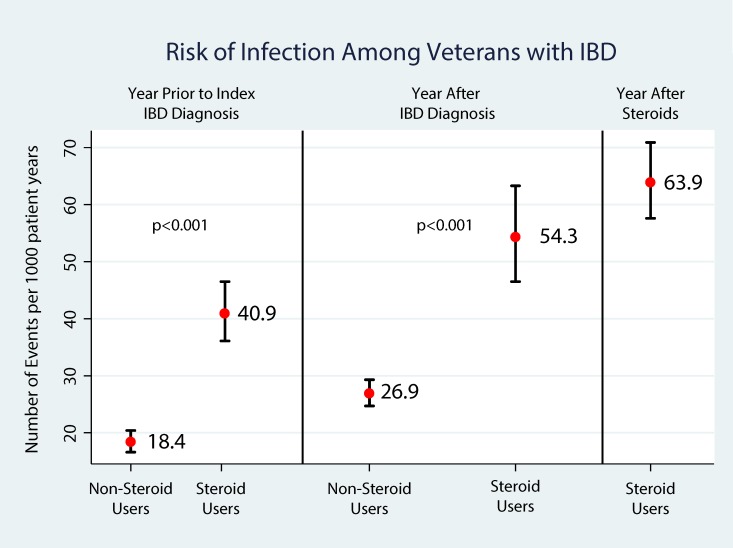
Results: Of the 30,456 Veterans with IBD, 32% required at least one course of corticosteroids during the study time period, and 17% of the steroid users had a prolonged course. Among these patients, only 26.2% underwent escalation of therapy. Patients visiting a gastroenterology (GI) physician were significantly more likely to receive corticosteroid-sparing medications. Factors associated with corticosteroid-sparing medications included younger age (OR = 0.96 per year,95%CI:0.95, 0.97), male gender (OR = 2.00,95%CI:1.16,3.46), GI visit during the corticosteroid evaluation period (OR = 8.01,95%CI:5.85,10.95) and the use of continuous corticosteroids vs. intermittent corticosteroids (OR = 2.28,95%CI:1.33,3.90). Rates of complications per 1000 person-years after IBD diagnosis were higher among corticosteroid users (venous thromboembolism [VTE] 9.0%; fragility fracture 2.6%; Infections 54.3) than non-corticosteroid users (VTE 4.9%; fragility fracture 1.9%; Infections 26.9). DEXA scan utilization rates among corticosteroid users were only 7.8%.
Conclusions: Prolonged corticosteroid therapy for the treatment of IBD is common and is associated with significant harm to patients. Patients with prolonged use of corticosteroids for IBD should be referred to gastroenterology early and universal efforts to improve the delivery of high quality care should be undertaken.
Conflict of interest statement
Figures
References
-
- Lukert BP, Raisz LG. Glucocorticoid-induced osteoporosis: pathogenesis and management. Annals of internal medicine. 1990;112(5):352–64. . - PubMed
-
- Higgins PD, Skup M, Mulani PM, Lin J, Chao J. Increased Risk of Venous Thromboembolic Events With Corticosteroid vs Biologic Therapy for Inflammatory Bowel Disease. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association. 2014. 10.1016/j.cgh.2014.07.017 . - DOI - PubMed
-
- Pearson DC, May GR, Fick GH, Sutherland LR. Azathioprine and 6-mercaptopurine in Crohn disease. A meta-analysis. Annals of internal medicine. 1995;123(2):132–42. . - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
