

Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial
- PMID: 27339115
- PMCID: PMC4961874
- DOI: 10.1016/S1470-2045(16)30102-4
Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial
Erratum in
-
Correction to Lancet Oncol 2016; 17:1055.Lancet Oncol. 2016 Aug;17(8):e321. doi: 10.1016/S1470-2045(16)30273-X. Epub 2016 Jun 24. Lancet Oncol. 2016. PMID: 27350346 Free PMC article. No abstract available.
Abstract
Background: Prostate cancer might have high radiation-fraction sensitivity that would give a therapeutic advantage to hypofractionated treatment. We present a pre-planned analysis of the efficacy and side-effects of a randomised trial comparing conventional and hypofractionated radiotherapy after 5 years follow-up.
Methods: CHHiP is a randomised, phase 3, non-inferiority trial that recruited men with localised prostate cancer (pT1b-T3aN0M0). Patients were randomly assigned (1:1:1) to conventional (74 Gy delivered in 37 fractions over 7·4 weeks) or one of two hypofractionated schedules (60 Gy in 20 fractions over 4 weeks or 57 Gy in 19 fractions over 3·8 weeks) all delivered with intensity-modulated techniques. Most patients were given radiotherapy with 3-6 months of neoadjuvant and concurrent androgen suppression. Randomisation was by computer-generated random permuted blocks, stratified by National Comprehensive Cancer Network (NCCN) risk group and radiotherapy treatment centre, and treatment allocation was not masked. The primary endpoint was time to biochemical or clinical failure; the critical hazard ratio (HR) for non-inferiority was 1·208. Analysis was by intention to treat. Long-term follow-up continues. The CHHiP trial is registered as an International Standard Randomised Controlled Trial, number ISRCTN97182923.
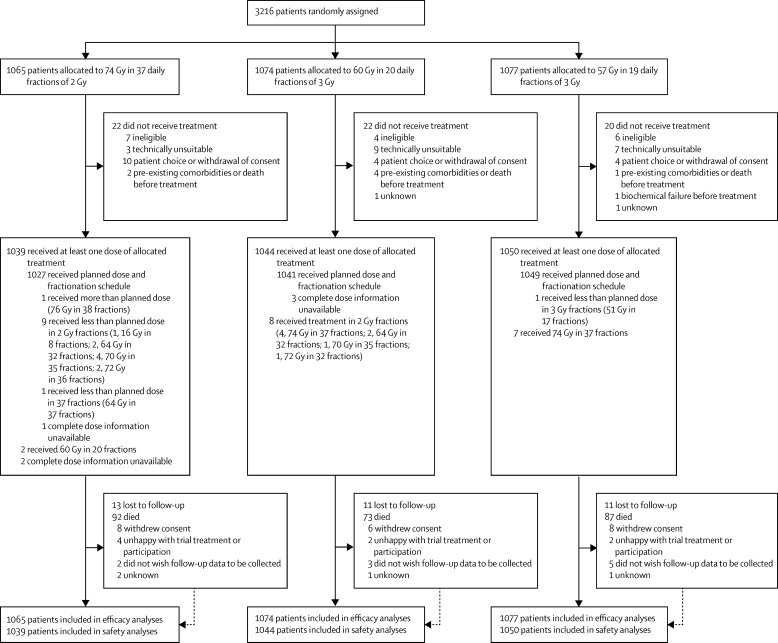
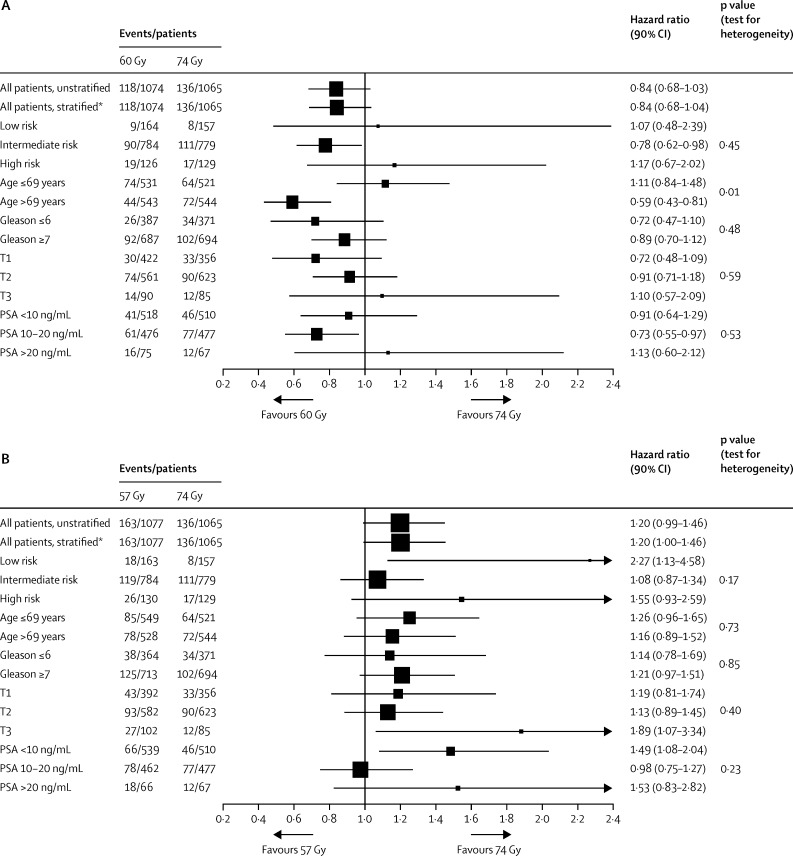
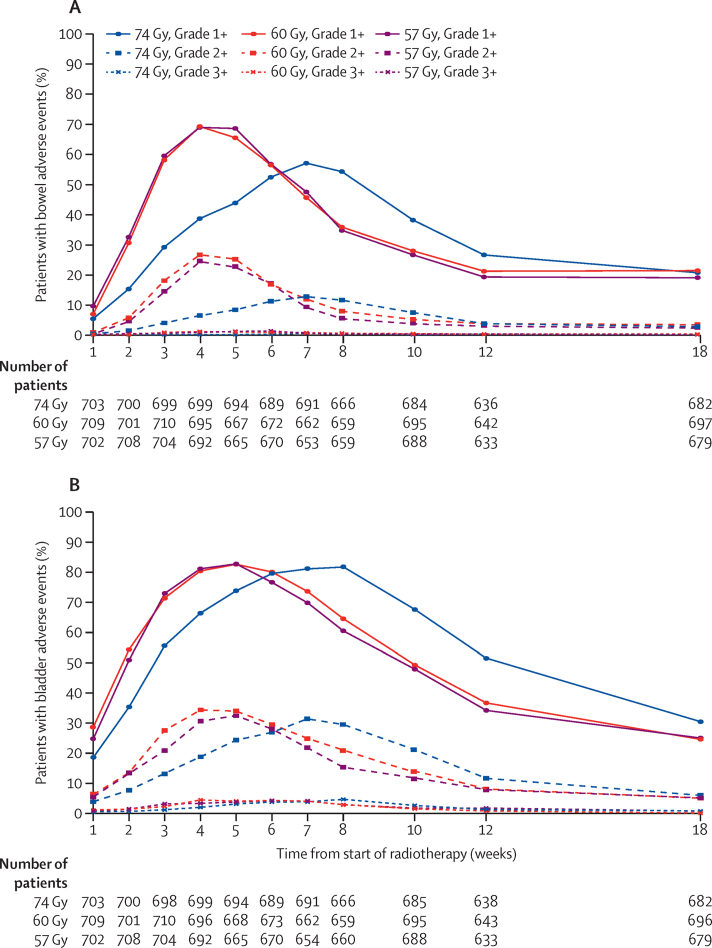
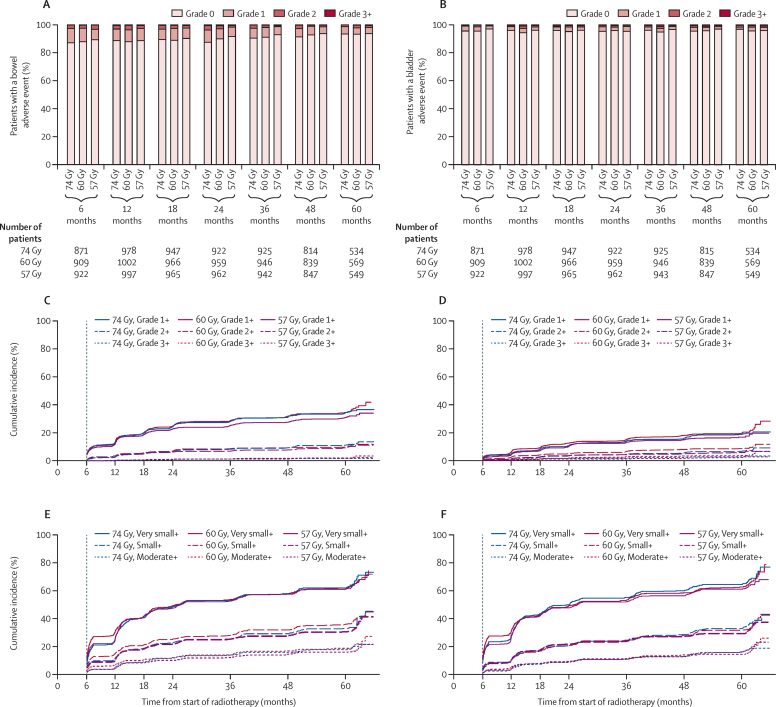
Findings: Between Oct 18, 2002, and June 17, 2011, 3216 men were enrolled from 71 centres and randomly assigned (74 Gy group, 1065 patients; 60 Gy group, 1074 patients; 57 Gy group, 1077 patients). Median follow-up was 62·4 months (IQR 53·9-77·0). The proportion of patients who were biochemical or clinical failure free at 5 years was 88·3% (95% CI 86·0-90·2) in the 74 Gy group, 90·6% (88·5-92·3) in the 60 Gy group, and 85·9% (83·4-88·0) in the 57 Gy group. 60 Gy was non-inferior to 74 Gy (HR 0·84 [90% CI 0·68-1·03], pNI=0·0018) but non-inferiority could not be claimed for 57 Gy compared with 74 Gy (HR 1·20 [0·99-1·46], pNI=0·48). Long-term side-effects were similar in the hypofractionated groups compared with the conventional group. There were no significant differences in either the proportion or cumulative incidence of side-effects 5 years after treatment using three clinician-reported as well as patient-reported outcome measures. The estimated cumulative 5 year incidence of Radiation Therapy Oncology Group (RTOG) grade 2 or worse bowel and bladder adverse events was 13·7% (111 events) and 9·1% (66 events) in the 74 Gy group, 11·9% (105 events) and 11·7% (88 events) in the 60 Gy group, 11·3% (95 events) and 6·6% (57 events) in the 57 Gy group, respectively. No treatment-related deaths were reported.
Interpretation: Hypofractionated radiotherapy using 60 Gy in 20 fractions is non-inferior to conventional fractionation using 74 Gy in 37 fractions and is recommended as a new standard of care for external-beam radiotherapy of localised prostate cancer.
Funding: Cancer Research UK, Department of Health, and the National Institute for Health Research Cancer Research Network.
Copyright © 2016 Dearnaley et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Hypofractionation for prostate cancer: tested and proven.Lancet Oncol. 2016 Aug;17(8):1020-1022. doi: 10.1016/S1470-2045(16)30150-4. Epub 2016 Jun 20. Lancet Oncol. 2016. PMID: 27339117 No abstract available.
-
Prostate Hypofractionated Radiotherapy Trial Results Need to be Interpreted with Caution due to Undertreatment of the Control Arm in the CHHiP Trial.Clin Oncol (R Coll Radiol). 2016 Dec;28(12):797. doi: 10.1016/j.clon.2016.08.008. Epub 2016 Aug 31. Clin Oncol (R Coll Radiol). 2016. PMID: 27591001 No abstract available.
-
Response to: Sivanandan et al. Prostate Hypofractionated Radiotherapy Trial Results Need to be Interpreted with Caution due to Undertreatment of the Control Arm in the CHHiP Trial.Clin Oncol (R Coll Radiol). 2016 Dec;28(12):798-799. doi: 10.1016/j.clon.2016.09.002. Epub 2016 Sep 15. Clin Oncol (R Coll Radiol). 2016. PMID: 27640308 No abstract available.
-
Prostate cancer: Moderate hypofractionated radiotherapy - not yet a standard of care.Nat Rev Clin Oncol. 2016 Nov;13(11):655-656. doi: 10.1038/nrclinonc.2016.147. Epub 2016 Sep 20. Nat Rev Clin Oncol. 2016. PMID: 27644320 No abstract available.
-
Hypofractionated radiotherapy for prostate cancer.Lancet Oncol. 2016 Dec;17(12):e517. doi: 10.1016/S1470-2045(16)30588-5. Lancet Oncol. 2016. PMID: 27924748 No abstract available.
-
Hypofractionated radiotherapy for prostate cancer - Authors' reply.Lancet Oncol. 2016 Dec;17(12):e518. doi: 10.1016/S1470-2045(16)30592-7. Lancet Oncol. 2016. PMID: 27924749 No abstract available.
-
Prostate cancer and hypofractionation: really a new standard of care?Transl Androl Urol. 2016 Dec;5(6):966-967. doi: 10.21037/tau.2016.08.19. Transl Androl Urol. 2016. PMID: 28078233 Free PMC article. No abstract available.
-
Six Questions to Ask Before We Shorten Radiation Treatments for Intact Prostate Cancer.Int J Radiat Oncol Biol Phys. 2017 Mar 15;97(4):718-721. doi: 10.1016/j.ijrobp.2016.11.038. Int J Radiat Oncol Biol Phys. 2017. PMID: 28244406 No abstract available.
References
-
- Cancer Research UK Prostate cancer statistics – key facts. 2015. http://info.cancerresearchuk.org/cancerstats/keyfacts/prostate-cancer/ (accessed Feb 1, 2016).
-
- Soerjomataram I, Lortet-Tieulent J, Parkin DM. Global burden of cancer in 2008: a systematic analysis of disability-adjusted life-years in 12 world regions. Lancet. 2012;380:1840–1850. - PubMed
-
- NCCN clinical practice guidelines in oncology (NCCN guidelines) for prostate cancer. 2011. http:\www.nccn.org (accessed Feb 1, 2016).
-
- Wolff RF, Ryder S, Bossi A. A systematic review of randomised controlled trials of radiotherapy for localised prostate cancer. Eur J Cancer. 2015;51:2345–2367. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
