

Acute pancreatitis complicated with deep vein thrombosis and pulmonary embolism: a case report
- PMID: 27339635
- PMCID: PMC4917977
- DOI: 10.1186/s13256-016-0968-6
Acute pancreatitis complicated with deep vein thrombosis and pulmonary embolism: a case report
Abstract
Background: Acute pancreatitis is an acute inflammatory process of the pancreas that can trigger a systemic inflammatory response. Pulmonary embolism refers to obstruction of the pulmonary artery or one of its branches by material (usually a thrombus) that originated elsewhere in the body. Extensive lower limb deep vein thrombosis with pulmonary embolism is a rare complication of acute pancreatitis that has been described in a few case reports. Deep vein thrombosis and hypercoagulable states in pancreatitis are thought to be due to release of pancreatic proteolytic enzymes from a cyst that is connected to the pancreatic duct and penetrates into a vessel. Proteolytic damage or inflammation of the vessels may also play a significant part. Acute pancreatitis also causes a systemic inflammatory response that has effects on an endothelium-dependent relaxing response for acetylcholine.
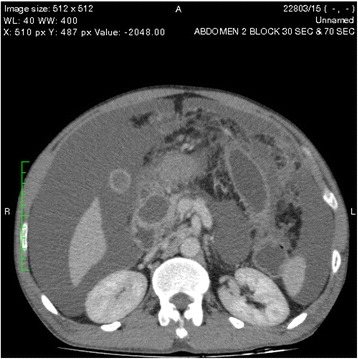
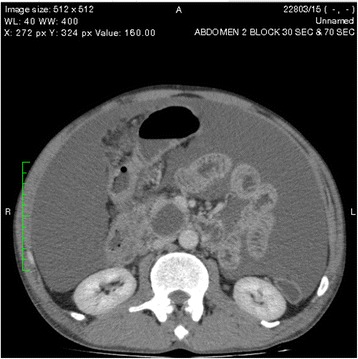
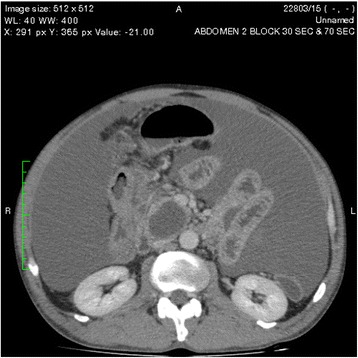
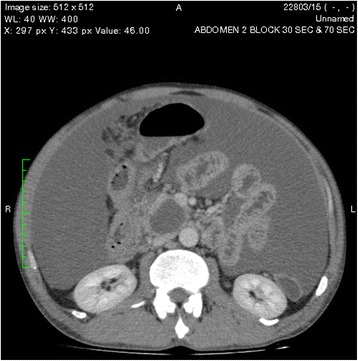
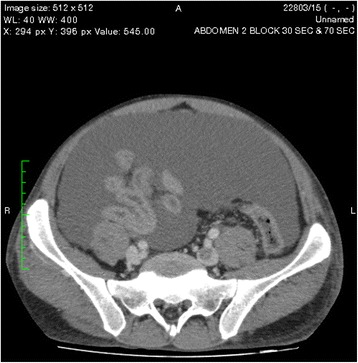
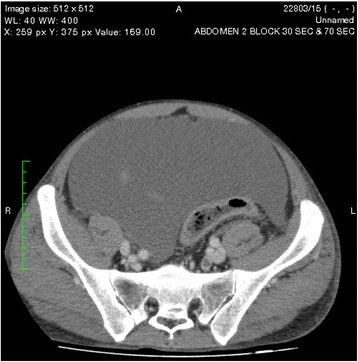
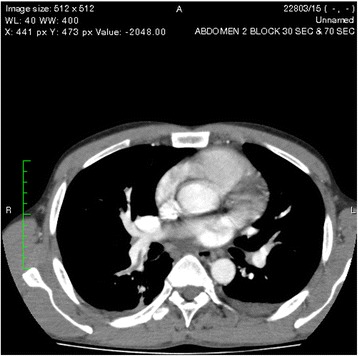
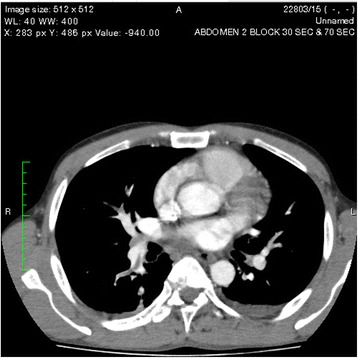
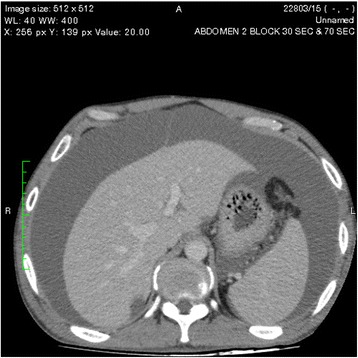
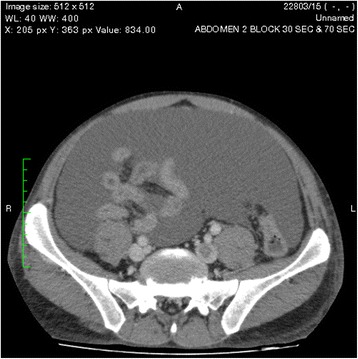
Case presentation: A 38-year-old Sri Lankan man presented with acute pancreatitis and later he developed progressive abdominal distention with bilateral ankle edema. A contrast-enhanced computed tomographic scan showed two pancreatic pseudocysts and deep vein thrombosis in both lower limbs, as well as a pulmonary embolism involving the right lower lobe pulmonary artery and the left segmental pulmonary arteries. One of the pseudocysts in the head of the pancreas was compressing the inferior vena cava without direct communication. The patient's thrombophilia screen result was negative. He was started on subcutaneous enoxaparin 1 mg/kg twice daily and warfarin to achieve a target international normalized ratio of 2-3.
Conclusions: Deep vein thrombosis with pulmonary embolism is a rare but life-threatening complication of acute pancreatitis. Once diagnosed, early treatment with intravenous heparin or thrombolysis is effective. Patients with severe acute pancreatitis may be at risk of deep vein thrombosis due to immobilization and other mechanisms, but anticoagulation as prophylaxis is often not used. However, it may be considered on a case-by-case basis in patients with pancreatitis who are acutely ill and immobilized, need intensive care unit admission, and have multiple risk factors for deep vein thromboembolism. Further studies must be undertaken to determine guidelines for deep vein thromboembolism prophylaxis in these patients.
Keywords: Acute pancreatitis; Case report; Deep vein thrombosis; Pulmonary embolism.
Figures
References
-
- Larvin M, et al. Assessment of clinical severity and prognosis. In: Beger HG, Warshaw AL, Büchler MW, et al., editors. The pancreas. Oxford: Blackwell; 1998. p. 489.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
