

[Preoperative Induction Therapy for Locally Advanced Thymic Tumors: A Retrospective Analysis Using the ChART Database]
- PMID: 27339721
- PMCID: PMC6133981
- DOI: 10.3779/j.issn.1009-3419.2016.07.06
[Preoperative Induction Therapy for Locally Advanced Thymic Tumors: A Retrospective Analysis Using the ChART Database]
Abstract
Background: To evaluate the role of preoperative induction therapy on prognosis of locally advanced thymic malignancies.
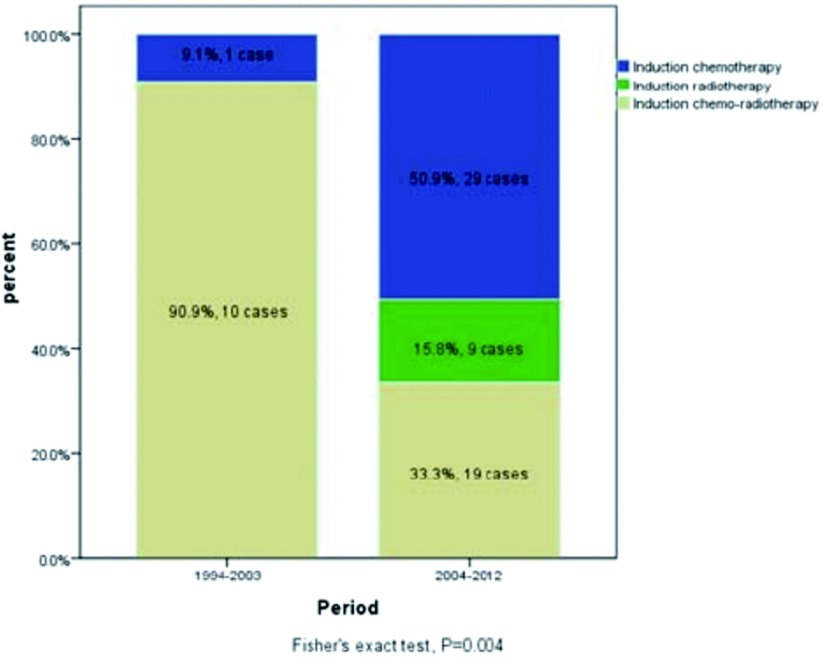
Methods: Between 1994 and 2012, patients received preoperative induction therapies (IT group) in the Chinese Alliance for Research in Thymomas (ChART) database, were compared with those having surgery directly after preoperative evaluation (DS group). All tumors receiving induction therapies were locally advanced (clinically stage III-IV) before treatment and those turned out to be in pathological stage I and II were considered downstaged by induction. Clinical pathological characteristics were retrospectively analyzed. To more accurately study the effect of induction therapies, stage IV patients were then excluded. Only stage I-III tumors in the IT group and stage III cases in the DS group were selected for further comparison in a subgroup analysis.
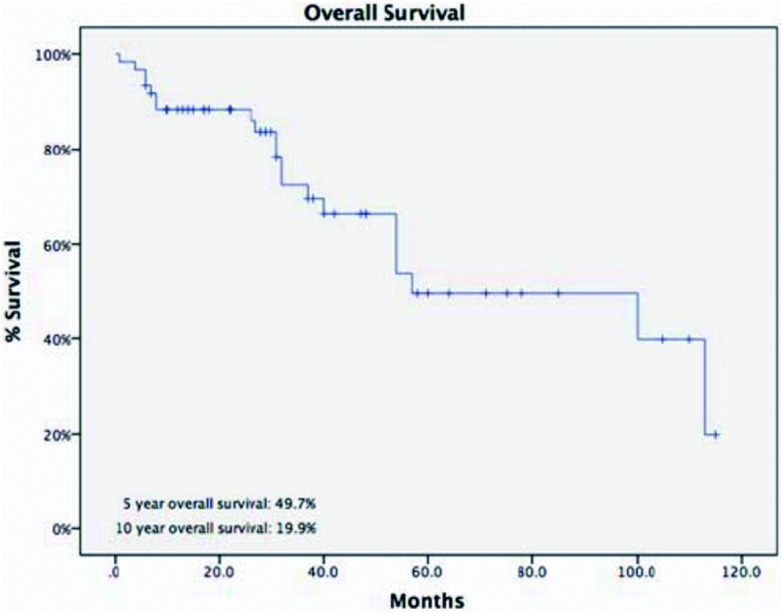
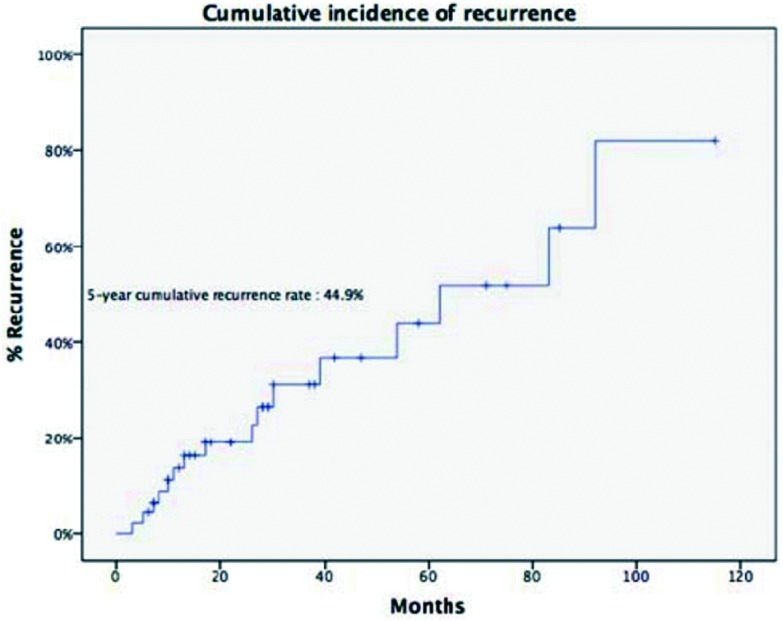
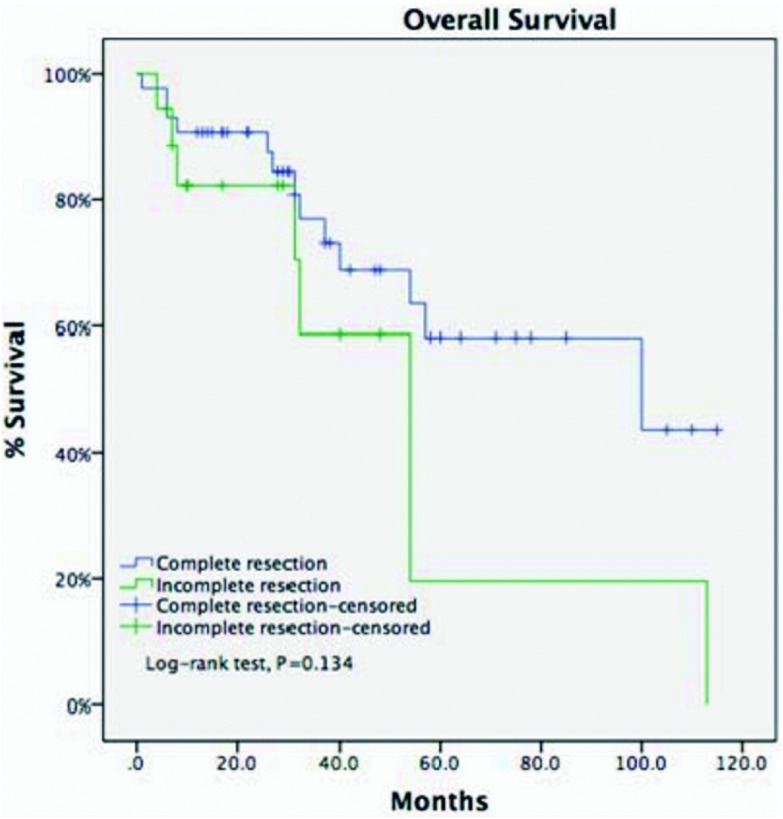
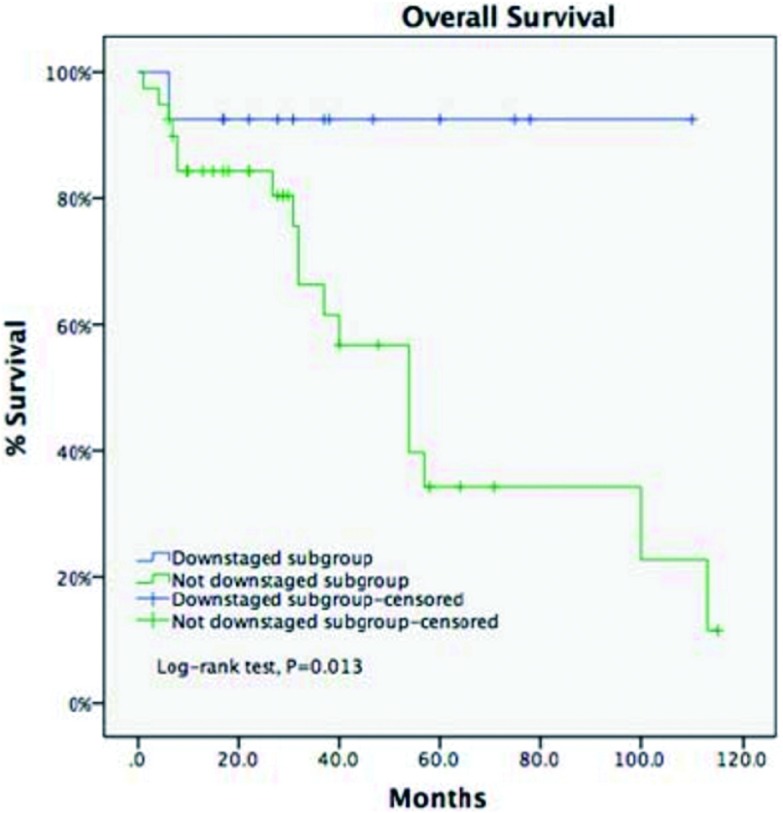
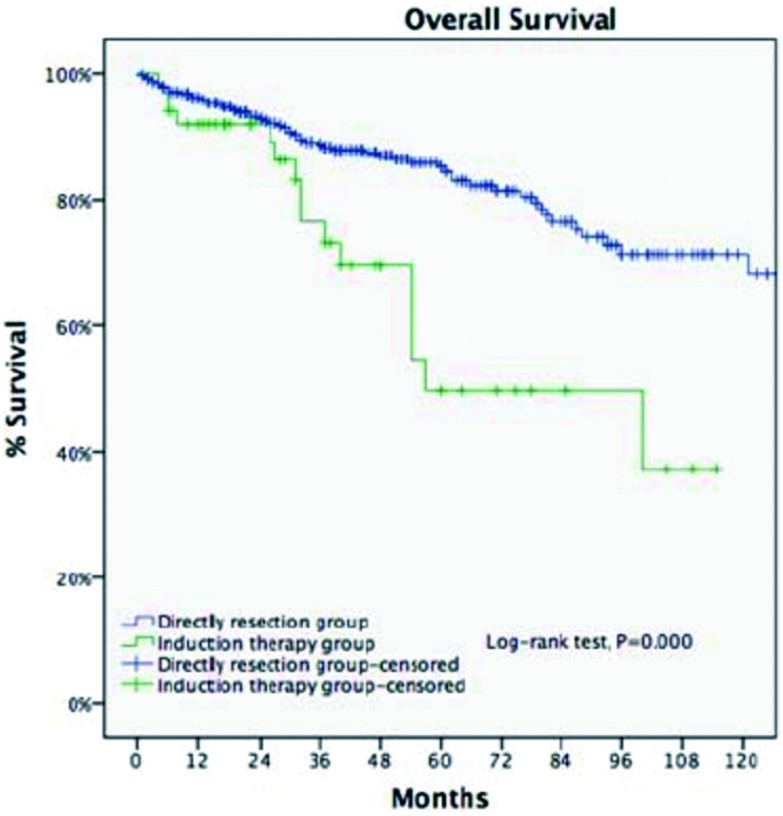
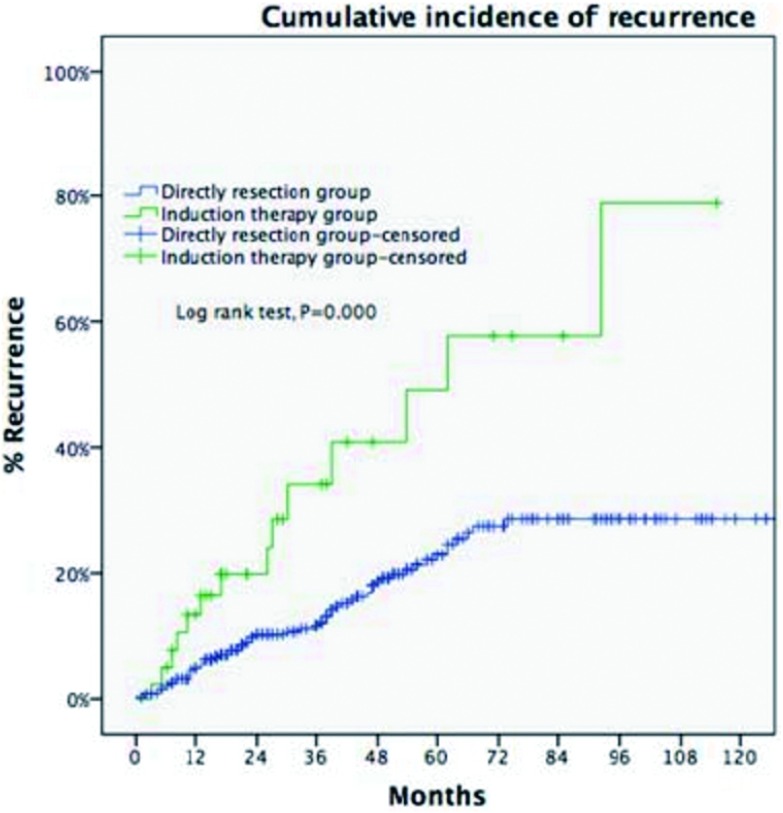
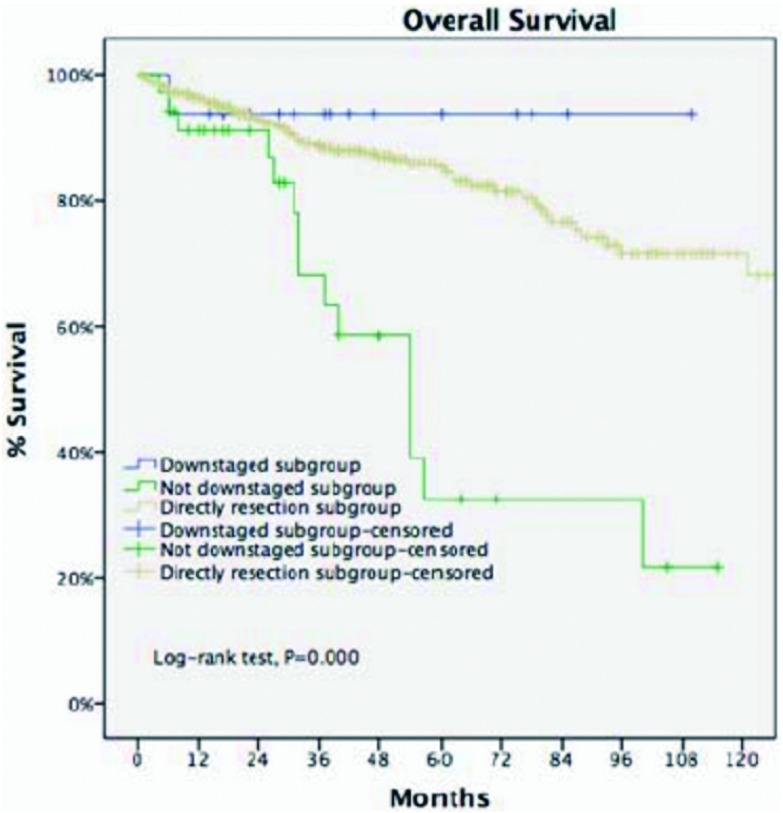
Results: Only 68 (4%) out of 1,713 patients had induction therapies, with a R0 resection of 67.6%, 5-year recurrence of 44.9%, and 5- and 10-year overall survivals (OS) of 49.7% and 19.9%. Seventeen patients (25%) were downstaged after induction. Significantly more thymomas were downstaged than thymic carcinomas (38.7% vs 13.9%, P=0.02). Tumors downstaged after induction had significantly higher 5-year OS than those not downstaged (93.8% vs 35.6%, P=0.013). For the subgroup analysis when stage IV patients were excluded, 5-year OS was 85.2% in the DS group and 68.1% in the IT group (P<0.001), although R0 resection were similar (76.4% vs 73.3%, P=0.63). However, 5-year OS in tumors downstaged after induction (93.8%) was similar to those in the DS group (85.2%, P=0.438), both significantly higher than those not downstaged after induction (35.6%, P<0.001).
Conclusions: Only 68 (4%) out of 1,713 patients had induction therapies, with a R0 resection of 67.6%, 5-year recurrence of 44.9%, and 5- and 10-year overall survivals (OS) of 49.7% and 19.9%. Seventeen patients (25%) were downstaged after induction. Significantly more thymomas were downstaged than thymic carcinomas (38.7% vs 13.9%, P=0.02). Tumors downstaged after induction had significantly higher 5-year OS than those not downstaged (93.8% vs 35.6%, P=0.013). For the subgroup analysis when stage IV patients were excluded, 5-year OS was 85.2% in the DS group and 68.1% in the IT group (P<0.001), although R0 resection were similar (76.4% vs 73.3%, P=0.63). However, 5-year OS in tumors downstaged after induction (93.8%) was similar to those in the DS group (85.2%, P=0.438), both significantly higher than those not downstaged after induction (35.6%, P<0.001). .
背景与目的 探讨术前诱导治疗在胸腺瘤中的应用及其对局部进展期胸腺瘤预后的影响。方法 收集中国胸腺肿瘤协作组(Chinese Alliance of Research for Thymomas, ChART)1994年1月1日至2012年12月31日回顾性数据库中局部进展期胸腺瘤(Masaoka-Koga分期为III期-IVa期)病例。分为诱导治疗组和直接手术组,对比分析两组的R0切除率、5年复发率及5年生存率等指标。诱导治疗组术后分期为Masaoka-Koga I期-II期的病例视为诱导治疗后降期。为更加精确评估诱导治疗效果,在剔除术后IV期病例的基础上,再次将诱导治疗组术后Masaoka-Koga I期-III期的病例与直接手术组Masaoka-Koga III期的病例进行对比分析。结果 ChART回顾性数据库1,713例有效病例中,局部进展期胸腺瘤706例,仅68例(4%)作了术前诱导治疗,R0切除率为67.6%,5年复发率为44.9%,5年与10年生存率分别为49.7%和19.9%。其中17例诱导治疗后达到降期,降期亚组中胸腺瘤的比例高于胸腺癌(38.7% vs 13.9%, P=0.02);与未降期亚组相比,降期亚组获得更高的5年生存率(93.8% vs 35.6%, P=0.013)。剔除术后IV期的病例后,直接手术组和诱导治疗组R0切除率接近(76.4% vs 73.3%, P=0.63),但5年生存率差异明显(85.2% vs 68.1%, P<0.001),对于降期亚组,5年生存率优于直接手术组(93.8% vs 85.2%, P=0.438),未降期亚组5年生存率仅35.6%,明显差于降期亚组和直接手术组(P<0.001)。结论 术前诱导治疗目前尚未在局部进展期胸腺瘤中广泛应用,但ChART的回顾性数据研究显示通过有效的术前诱导治疗可以使难以彻底切除的病例降期后增加R0切除的机会,从而延长生存,特别是胸腺瘤的病例。这一初步结果将有助于未来的研究。.
Figures
Similar articles
-
Preoperative induction therapy for locally advanced thymic tumors: a retrospective analysis using the ChART database.J Thorac Dis. 2016 Apr;8(4):665-72. doi: 10.21037/jtd.2016.03.02. J Thorac Dis. 2016. PMID: 27114833 Free PMC article.
-
[Pretreatment Biopsy for Histological Diagnosis and Induction Therapy in Thymic Tumors].Zhongguo Fei Ai Za Zhi. 2016 Jul 20;19(7):437-44. doi: 10.3779/j.issn.1009-3419.2016.07.05. Zhongguo Fei Ai Za Zhi. 2016. PMID: 27339720 Free PMC article. Chinese.
-
[Application of Postoperative Chemotherapy on Thymomas and Its Prognostic Effect].Zhongguo Fei Ai Za Zhi. 2016 Jul 20;19(7):473-82. doi: 10.3779/j.issn.1009-3419.2016.07.10. Zhongguo Fei Ai Za Zhi. 2016. PMID: 27339725 Free PMC article. Chinese.
-
Treatment of advanced thymoma and thymic carcinoma.Curr Treat Options Oncol. 2008 Dec;9(4-6):277-87. doi: 10.1007/s11864-009-0083-7. Epub 2009 Apr 21. Curr Treat Options Oncol. 2008. PMID: 19381821 Free PMC article. Review.
-
Natural history and treatment of malignant thymoma.Oncology (Williston Park). 1998 Jul;12(7):1001-5; discussion 1006. Oncology (Williston Park). 1998. PMID: 9684271 Review.
Cited by
-
Clinical Outcomes of Thymic Carcinoma: The Role of Radiotherapy Combined with Multimodal Treatments.Cancers (Basel). 2023 Apr 12;15(8):2262. doi: 10.3390/cancers15082262. Cancers (Basel). 2023. PMID: 37190190 Free PMC article.
References
-
- Riely GJ, Huang J. Induction therapy for locally advanced thymoma. http://med.wanfangdata.com.cn/Paper/Detail/PeriodicalPaper_PM20859127. J Thorac Oncol. 2010;5(10 Suppl 4):S323–S326. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
