

[Outcome of Nonsurgical Treatment for Locally Advanced Thymic Tumors]
- PMID: 27339726
- PMCID: PMC6133979
- DOI: 10.3779/j.issn.1009-3419.2016.07.11
[Outcome of Nonsurgical Treatment for Locally Advanced Thymic Tumors]
Abstract
Background: Surgical resection remains the mainstay of treatment for patients with early-staged thymic tumors, while chemotherapy is most commonly used in stage IV cases. As for locally advanced thymic tumors, especially those unsuitable for surgery, the optimal therapy is still controversial. Thus, we conducted this retrospective study by comparing three nonsurgical treatment modalities to find some clues.
Methods: Three treatment modalities were used in 42 patients from October 2000 to December 2010, including radiotherapy (RT) alone, sequential chemoradiation (SCRT) and concurrent chemoradiation (CCRT). Objective response rate (ORR), overall survival (OS) and toxicity of the three regimens were compared accordingly.
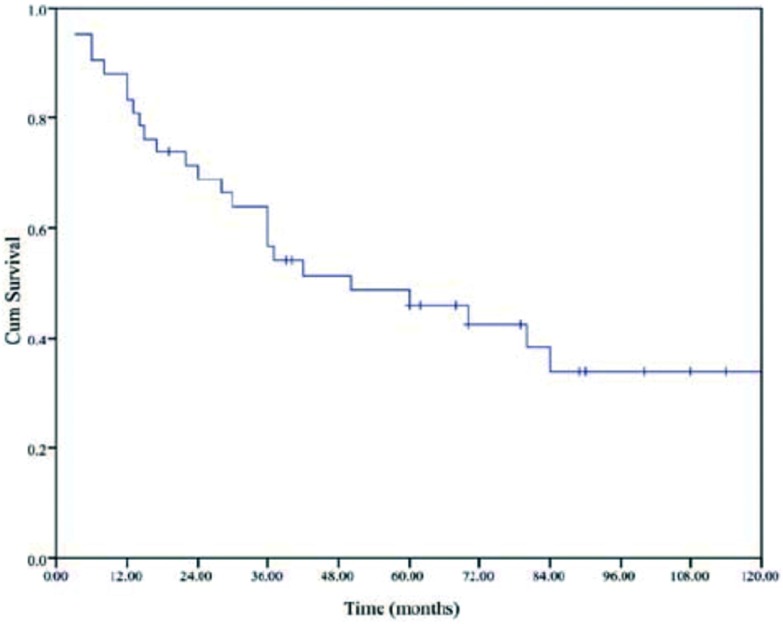
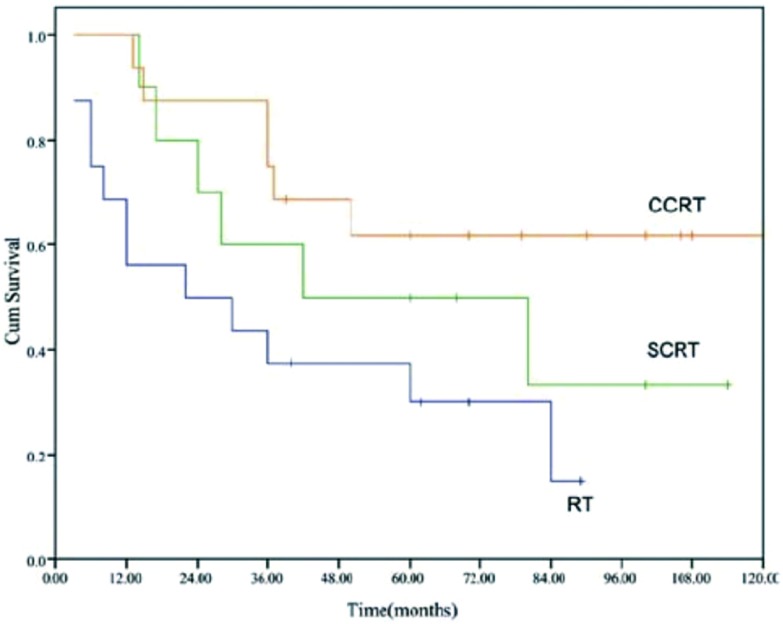
Results: The ORR in all 42 patients was 61.9%, and 5-year OS was 46%. The ORR of RT, SCRT and CCRT were 43.8%, 50% and 87.5%, respectively (RT vs SCRT, P=0.692; RT vs CCRT, P=0.009; SCRT vs CCRT, P=0.051). The 5-year OS of RT, SCRT and CCRT were 30%, 50% and 61.9%, respectively (RT vs SCRT, P=0.230; RT vs CCRT, P=0.011; SCRT vs CCRT, P=0.282). Eleven patients developed neutropenia of grade 3-4, with 7 in CCRT group and 4 in SCRT, respectively. Nine patients experienced esophagitis of grade 3 with 2 in RT, 3 in SCRT and 4 in CCRT. There were also two cases of grade 3 radiation induced pneumonitis in CCRT group. No life-threatening side effects were noted.
Conclusions: When used to treat locally advanced thymic tumors unsuitable for surgery, CCRT performed more favorably than RT alone or SCRT in both tumor response and long time survival, but probably with the increasing risk of pulmonary damage. CCRT may offer the best chance of disease control in the management of locally advanced disease.
背景与目的 手术切除是早期胸腺肿瘤的主要治疗方法,而对于IV期的病变,化疗则是最常用的方案。对于局部晚期的肿瘤,尤其是不适合手术的病例,何种治疗方案效果更优则没有明确的结论。鉴于此,我们做了这项回顾性的研究,通过对三种非手术疗法的比较,希望找到一些线索。方法 自2000年10月至2010年12月,共有42例患者接受了三种非手术方案的治疗。这三种模式分别是单独放疗(radiotherapy, RT)、序贯化放疗(sequential chemoradiation, SCRT)以及同步放化疗(concurrent chemoradiation, CCRT)。并对三种方案的缓解率(objective response rate, ORR)、总生存期(overall survival, OS)以及治疗的相关毒副反应进行比较。结果 全组42例患者中,总的缓解率为61.9%,5年生存率为46%。RT组、SCRT组以及CCRT组的缓解率分别是43.8%、50%和87.5%(RT vs SCRT, P=0.692; RT vs CCRT, P=0.009; SCRT vs CCRT, P=0.051)。RT组、SCRT组以及CCRT组的5年生存率分别是30%、50%和61.9%(RT vs SCRT, P=0.230; RT vs CCRT, P=0.011; SCRT vs CCRT, P=0.282)。共有11例患者发生了3度-4度的中性粒细胞减少,其中7例出现在CCRT组,另4例出现在SCRT组。有9例患者主诉有3度放射性食道炎,其中RT组2例,SCRT组3例,CCRT组4例。另外,CCRT组还出现了2例3度的放射性肺炎。未发现致命的5度毒副反应。结论 在治疗不适合手术的局部晚期胸腺肿瘤上,CCRT显示出了比RT和CCRT更好的局部控制以及长期生存优势,不过也有增加肺损伤风险的可能。对于局部侵袭性的胸腺肿瘤,CCRT可提供最佳的肿瘤控制效果。.
Figures
Similar articles
-
Outcome of nonsurgical treatment for locally advanced thymic tumors.J Thorac Dis. 2016 Apr;8(4):705-10. doi: 10.21037/jtd.2016.01.79. J Thorac Dis. 2016. PMID: 27114838 Free PMC article.
-
[Concurrent chemoradiotherapy followed by consolidation chemotherapy and sequential chemoradiotherapy for stage III non-small cell lung cancer: comparison in 93 patients].Nan Fang Yi Ke Da Xue Xue Bao. 2012 Mar;32(3):362-7. Nan Fang Yi Ke Da Xue Xue Bao. 2012. PMID: 22445984 Chinese.
-
Prognosis of Concurrent Versus Sequential Chemo-Radiotherapy Induction Followed by Surgical Resection in Patients with Advanced Thymic Epithelial Tumors: A Retrospective Study.Ann Surg Oncol. 2023 Oct;30(11):6739-6747. doi: 10.1245/s10434-023-13954-x. Epub 2023 Jul 15. Ann Surg Oncol. 2023. PMID: 37454019
-
Sequential chemotherapy after definitive radiotherapy in markedly elderly patients with advanced esophageal cancer.Indian J Cancer. 2022 Apr-Jun;59(2):244-250. doi: 10.4103/ijc.IJC_768_19. Indian J Cancer. 2022. PMID: 33402604 Review.
-
Thymic Malignancy-Updates in Staging and Management.Surg Oncol Clin N Am. 2020 Oct;29(4):581-601. doi: 10.1016/j.soc.2020.06.010. Epub 2020 Aug 11. Surg Oncol Clin N Am. 2020. PMID: 32883460 Review.
References
-
- Kondo K, Monden Y. Therapy for thymic epithelial tumors: a clinical study of 1, 320 patients from Japan. https://www.researchgate.net/publication/10577036_Therapy_for_thymic_epi.... Ann Thorac Surg. 2003;76(3):878–884. - PubMed
-
- Riely GJ, Huang J. Induction therapy for locally advanced thymoma. J Thorac Oncol. 2010;5(suppl 4):S323–S236. - PubMed
-
- Benveniste MF, Korst RJ, Rajan A, et al. A practical guide from the International Thymic Malignancy Interest Group (ITMIG) regarding the radiographic assessment of treatment response of thymic epithelial tumors using modified RECIST criteria. J Thorac Oncol. 2014;9(suppl 2):S119–S124. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
