

Shear Stiffness of 4 Common Intracranial Tumors Measured Using MR Elastography: Comparison with Intraoperative Consistency Grading
- PMID: 27339950
- PMCID: PMC7960472
- DOI: 10.3174/ajnr.A4832
Shear Stiffness of 4 Common Intracranial Tumors Measured Using MR Elastography: Comparison with Intraoperative Consistency Grading
Abstract
Background and purpose: The stiffness of intracranial tumors affects the outcome of tumor removal. We evaluated the stiffness of 4 common intracranial tumors by using MR elastography and tested whether MR elastography had the potential to discriminate firm tumors preoperatively.
Materials and methods: Thirty-four patients with meningiomas, pituitary adenomas, vestibular schwannomas, and gliomas scheduled for resection were recruited for MR elastography. On the elastogram, the mean and the maximum shear stiffnesses were measured by placing an ROI on the tumor. Blinded to the MR elastography findings, surgeons conducted qualitative intraoperative assessment of tumor consistency by using a 5-point scale. Histopathologic diagnosis was confirmed by using the resected specimens. The mean and maximum shear stiffnesses were compared with histopathologic subtypes, and the intraoperative tumor consistency was graded by the surgeons.
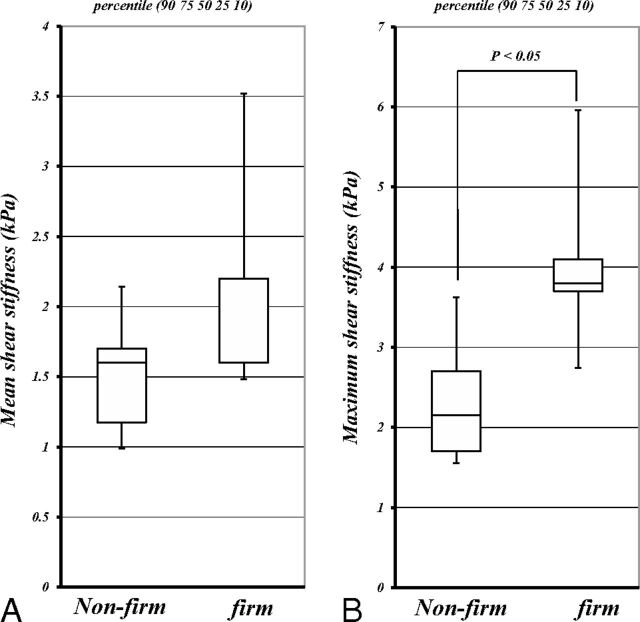
Results: The mean and maximum shear stiffnesses were the following: 1.9 ± 0.8 kPa and 3.4 ± 1.5 kPa for meningiomas, 1.2 ± 0.3 kPa and 1.8 ± 0.5 kPa for pituitary adenomas, 2.0 ± 0.4 kPa and 2.7 ± 0.8 kPa for vestibular schwannomas, and 1.5 ± 0.2 kPa and 2.7 ± 0.8 kPa for gliomas. The mean and maximum shear stiffnesses for meningiomas were higher than those of pituitary adenomas (P < .05). The mean and maximum shear stiffnesses were significantly correlated with the surgeon's qualitative assessment of tumor consistency (P < .05). The maximum shear stiffness for 5 firm tumors was higher than that of nonfirm tumors (P < .05).
Conclusions: MR elastography could evaluate intracranial tumors on the basis of their physical property of shear stiffness. MR elastography may be useful in discriminating firm tumors preoperatively.
© 2016 by American Journal of Neuroradiology.
Figures






Similar articles
-
Predicting pituitary adenoma consistency with preoperative magnetic resonance elastography.J Neurosurg. 2021 Oct 29;136(5):1356-1363. doi: 10.3171/2021.6.JNS204425. Print 2022 May 1. J Neurosurg. 2021. PMID: 34715659 Free PMC article.
-
Relationship between Shear Stiffness Measured by MR Elastography and Perfusion Metrics Measured by Perfusion CT of Meningiomas.AJNR Am J Neuroradiol. 2021 Jul;42(7):1216-1222. doi: 10.3174/ajnr.A7117. Epub 2021 May 13. AJNR Am J Neuroradiol. 2021. PMID: 33985944 Free PMC article.
-
Use of magnetic resonance elastography to gauge meningioma intratumoral consistency and histotype.Neuroimage Clin. 2022;36:103173. doi: 10.1016/j.nicl.2022.103173. Epub 2022 Aug 29. Neuroimage Clin. 2022. PMID: 36081257 Free PMC article.
-
In Vivo Measurement of Brain Tumor Elasticity Using Intraoperative Shear Wave Elastography.Ultraschall Med. 2016 Dec;37(6):584-590. doi: 10.1055/s-0034-1399152. Epub 2015 Apr 15. Ultraschall Med. 2016. PMID: 25876221 English.
-
Shear wave elastography in diffuse thyroid disease.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2021 Jun;165(2):152-156. doi: 10.5507/bp.2020.018. Epub 2020 May 5. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2021. PMID: 32394978
Cited by
-
Mechanical Properties of the Extracellular Environment of Human Brain Cells Drive the Effectiveness of Drugs in Fighting Central Nervous System Cancers.Brain Sci. 2022 Jul 15;12(7):927. doi: 10.3390/brainsci12070927. Brain Sci. 2022. PMID: 35884733 Free PMC article. Review.
-
MR Elastography Analysis of Glioma Stiffness and IDH1-Mutation Status.AJNR Am J Neuroradiol. 2018 Jan;39(1):31-36. doi: 10.3174/ajnr.A5415. Epub 2017 Oct 26. AJNR Am J Neuroradiol. 2018. PMID: 29074637 Free PMC article.
-
Applications of elastography in operative neurosurgery: A systematic review.J Clin Neurosci. 2022 Oct;104:18-28. doi: 10.1016/j.jocn.2022.07.019. Epub 2022 Aug 4. J Clin Neurosci. 2022. PMID: 35933785 Free PMC article.
-
Supershear Rayleigh wave imaging for quantitative assessment of biomechanical properties of brain using air-coupled optical coherence elastography.APL Bioeng. 2023 Oct 30;7(4):046107. doi: 10.1063/5.0160213. eCollection 2023 Dec. APL Bioeng. 2023. PMID: 37915751 Free PMC article.
-
Stiffness and Beyond: What MR Elastography Can Tell Us About Brain Structure and Function Under Physiologic and Pathologic Conditions.Top Magn Reson Imaging. 2018 Oct;27(5):305-318. doi: 10.1097/RMR.0000000000000178. Top Magn Reson Imaging. 2018. PMID: 30289827 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources