

A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (Tacrolimus) Formulations (ASTCOFF): An Open-Label, Prospective, Randomized, Two-Arm, Three-Period Crossover Study
- PMID: 27340950
- PMCID: PMC5297985
- DOI: 10.1111/ajt.13935
A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (Tacrolimus) Formulations (ASTCOFF): An Open-Label, Prospective, Randomized, Two-Arm, Three-Period Crossover Study
Abstract
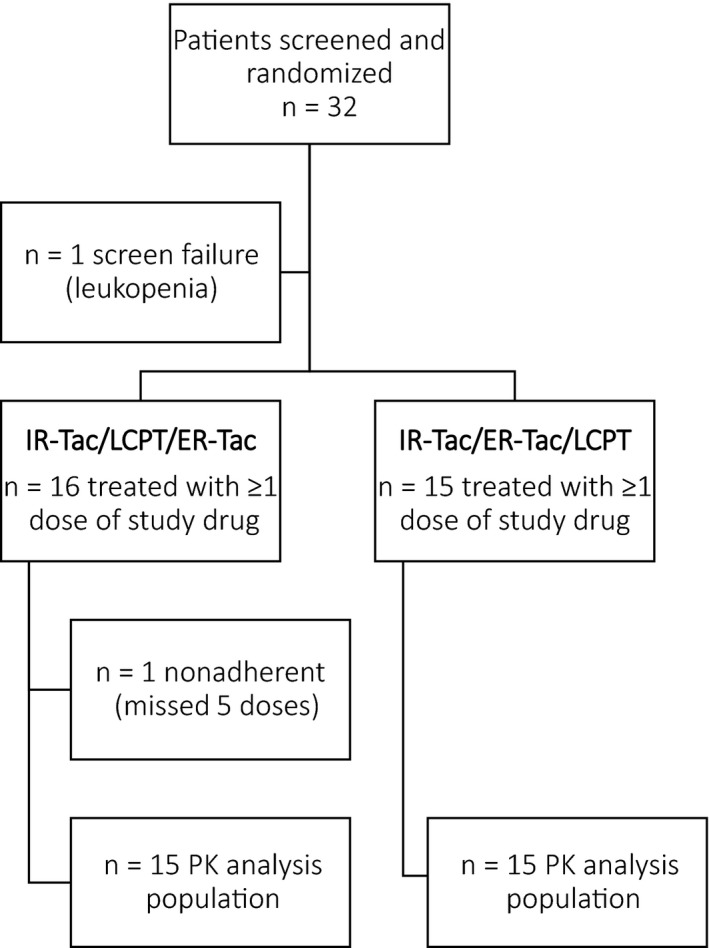
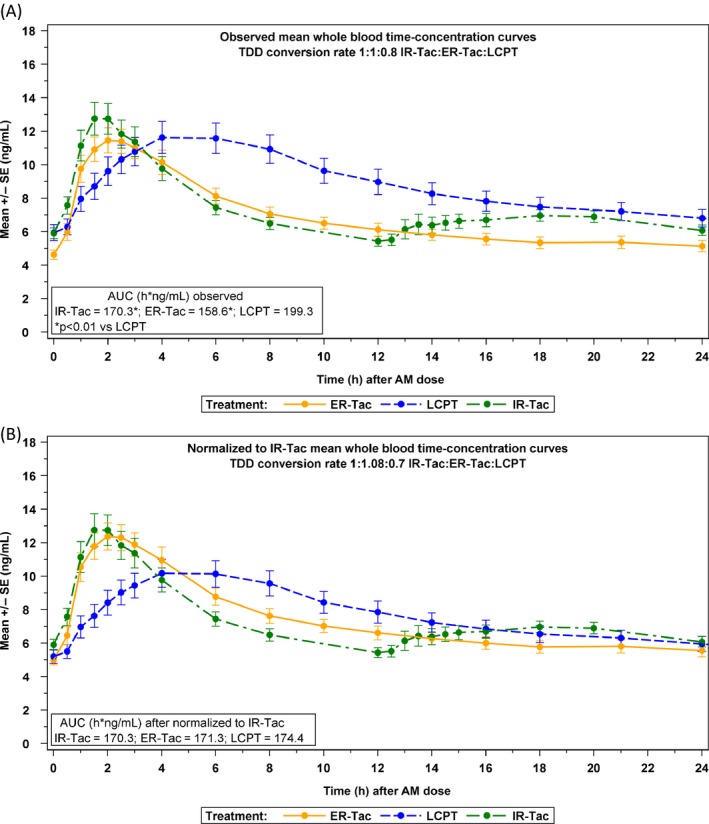
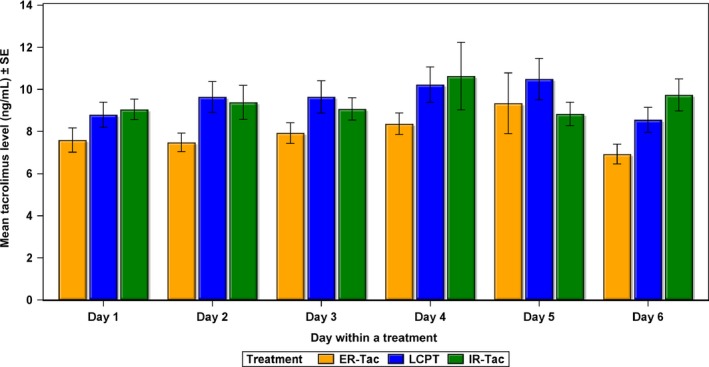
This two-sequence, three-period crossover study is the first pharmacokinetic (PK) study to compare all three innovator formulations of tacrolimus (twice-daily immediate-release tacrolimus capsules [IR-Tac]; once-daily extended-release tacrolimus capsules [ER-Tac]; novel once-daily tacrolimus tablets [LCPT]). Stable renal transplant patients were dosed with each drug for 7 days, and blood samples were obtained over 24 h. Thirty subjects were included in the PK analysis set. A conversion factor of 1:1:0.80 for IR-Tac:ER-Tac:LCPT was used; no dose adjustments were permitted during the study. The median (interquartile range) total daily dose was 6.0 (4.0-8.0) mg for IR-Tac and ER-Tac and 4.8 (3.3-6.3) for LCPT. Significantly higher exposure on a per milligram basis, lower intraday fluctuation and prolonged time (Tmax ) to peak concentration (Cmax ) were found for LCPT versus IR-Tac or ER-Tac. ER-Tac showed no differences versus IR-Tac in exposure, Cmax , Tmax or fluctuation. The observed exposure of IR-Tac was used to normalize exposure for LCPT and ER-Tac, resulting in the following recommended total daily dose conversion rates: IR-Tac:ER-Tac, +8%; IR-Tac:LCPT, -30%; ER-Tac:LCPT, -36%. After exposure normalization, Cmax was ~17% lower for LCPT than for IR-Tac or ER-Tac; Cmin was ~6% lower for LCPT compared with IR-Tac and 3% higher compared with ER-Tac.
Trial registration: ClinicalTrials.gov NCT02339246.
Keywords: calcineurin inhibitor: tacrolimus; clinical research/practice; clinical trial; immunosuppressant; kidney transplantation/nephrology; pharmacokinetics/pharmacodynamics.
© 2016 The Authors. American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of American Society of Transplant Surgeons.
Figures

Comment in
-
Fluctuation Does Not Mean Variability: A Pharmacokinetic Point of View.Am J Transplant. 2017 Jun;17(6):1691-1692. doi: 10.1111/ajt.14237. Epub 2017 Mar 17. Am J Transplant. 2017. PMID: 28226402 No abstract available.
-
Reply to "Fluctuation Does Not Mean Variability: A Pharmacokinetic Point of View".Am J Transplant. 2017 Jun;17(6):1693. doi: 10.1111/ajt.14248. Epub 2017 Mar 22. Am J Transplant. 2017. PMID: 28248455 No abstract available.
References
-
- Hart A, Smith JM, Skeans MA, et al. OPTN/SRTR annual data report 2014: Kidney. Am J Transplant 2016; 16(Suppl 2): 11–46. - PubMed
-
- Silva HT, Yang HC, Abouljoud M, et al. One‐year results with extended‐release tacrolimus/MMF, tacrolimus/MMF and cyclosporine/MMF in de novo kidney transplant recipients. Am J Transplant 2007; 7: 595–608. - PubMed
-
- Krämer BK, Charpentier B, Bäckman L, et al. Tacrolimus once daily (ADVAGRAF) versus twice daily (PROGRAF) in de novo renal transplantation: A randomized phase III study. Am J Transplant 2010; 10: 2632–2643. - PubMed
-
- Alloway R, Steinberg S, Khalil K, et al. Conversion of stable kidney transplant recipients from a twice daily Prograf‐based regimen to a once daily modified release tacrolimus‐based regimen. Transplant Proc 2005; 37: 867–870. - PubMed
-
- Slatinska J, Rohal T, Wohlfahrtova M, Viklicky O. Long‐term follow‐up of stable kidney transplant recipients after conversion from tacrolimus twice daily immediate release to tacrolimus once‐daily prolonged release: A large single‐center experience. Transplant Proc 2013; 45: 1491–1496. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
