

Treatment Patterns with Antidementia Drugs in the United States: Medicare Cohort Study
- PMID: 27341454
- PMCID: PMC5045869
- DOI: 10.1111/jgs.14226
Treatment Patterns with Antidementia Drugs in the United States: Medicare Cohort Study
Abstract
Objectives: To evaluate frequency of use of two anti-dementia drug classes approved for treatment of symptoms, whether populations most likely to benefit are treated, and correlates of treatment initiation.
Design: Nationally representative cohort study.
Setting: Fee-for-service Medicare.
Participants: Elderly adults with dementia enrolled in Medicare Parts A, B, and D in 2009 (N = 433,559) and a subset with incident dementia (n = 185,449).
Measurements: Main outcome was any prescription fill for antidementia drugs (cholinesterase inhibitors (ChEIs) or memantine) within 1 year.
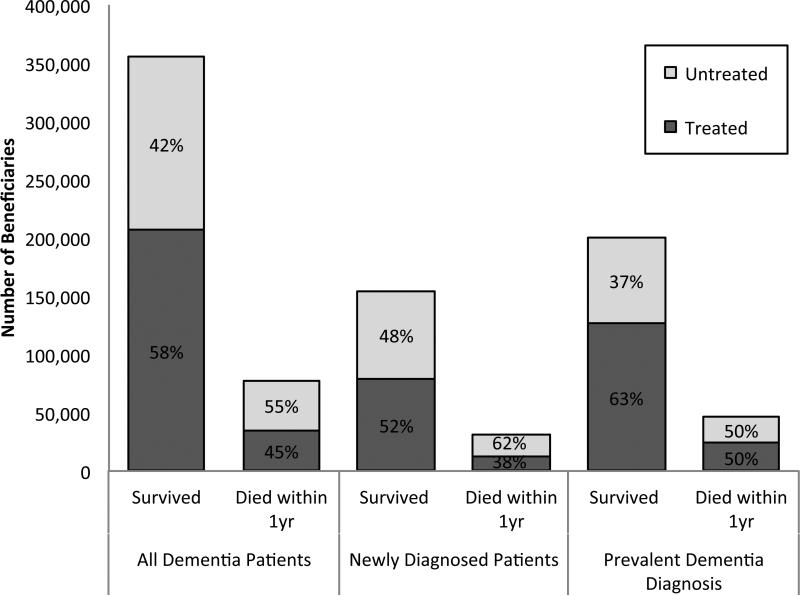
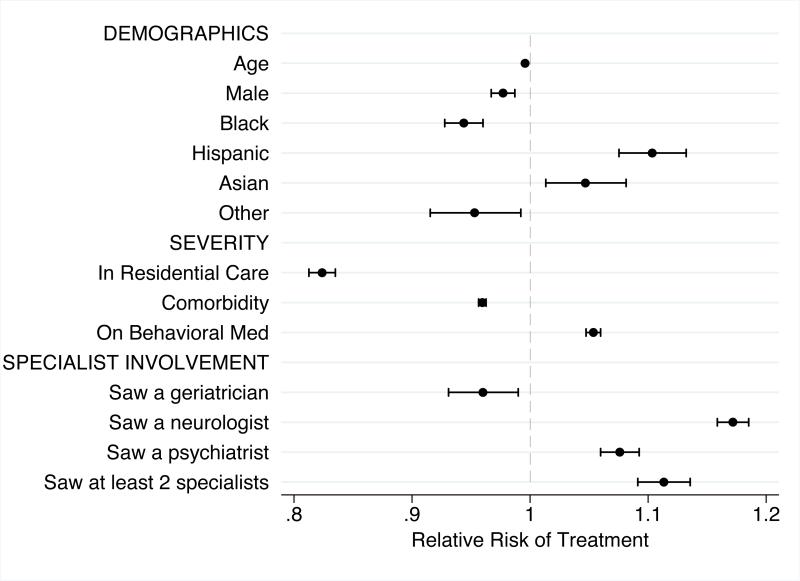
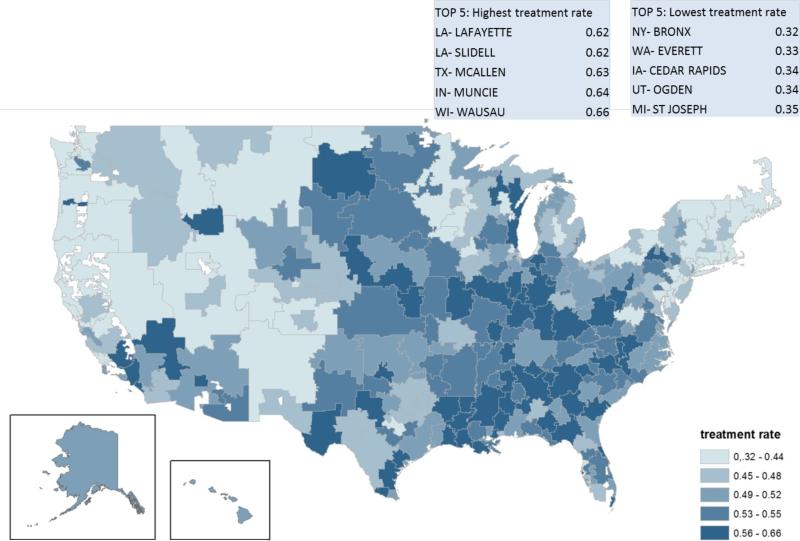
Results: Treatment with antidementia drugs occurred in 55.8% of all participants with dementia and 49.3% of those with incident dementia. There was no difference between ChEIs and memantine use according to dementia severity (measured as death within first year or living in residential care vs in a community setting) even though memantine is not indicated in mild disease. In incident cases, initiation of treatment was lower in residential care (relative risk (RR) = 0.82, 95% confidence interval (CI) = 0.81-0.83) and with more comorbidities (RR = 0.96, 95% CI = 0.96-0.96). Sixty percent of participants were managed in primary care alone. Seeing a neurologist (RR = 1.07, 95% CI = 1.06-1.09) or psychiatrist (RR = 1.17, 95% CI = 1.16-1.19) was associated with higher likelihood of treatment than seeing a primary care provider alone, and seeing geriatrician was associated with with lower likelihood (RR = 0.96, 95% CI = 0.93-0.99). Across the United States, the proportion of newly diagnosed individuals started on antidementia treatment varied from 32% to 66% across hospital referral regions.
Conclusion: Antidementia drugs are used less often in people with late disease, but there is no differentiation in medication choice. Although primary care providers most often prescribe antidementia medication without specialty support, differences in practice between specialties are evident.
Keywords: Medicare; dementia; drug treatment.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Figures
Similar articles
-
Effect of Medicare Part D on Ethnoracial Disparities in Antidementia Medication Use.J Am Geriatr Soc. 2018 Sep;66(9):1760-1767. doi: 10.1111/jgs.15494. Epub 2018 Aug 10. J Am Geriatr Soc. 2018. PMID: 30095169
-
Racial and Ethnic Differences in Initiation and Discontinuation of Antidementia Drugs by Medicare Beneficiaries.J Am Geriatr Soc. 2016 Sep;64(9):1806-14. doi: 10.1111/jgs.14403. Epub 2016 Aug 22. J Am Geriatr Soc. 2016. PMID: 27549029 Free PMC article.
-
The impact of Medicare prescription drug coverage on the use of antidementia drugs.BMC Geriatr. 2013 Apr 27;13:37. doi: 10.1186/1471-2318-13-37. BMC Geriatr. 2013. PMID: 23621892 Free PMC article.
-
Withdrawal of Antidementia Drugs in Older People: Who, When and How?Drugs Aging. 2016 Aug;33(8):545-56. doi: 10.1007/s40266-016-0384-z. Drugs Aging. 2016. PMID: 27393698 Review.
-
Contemporary issues in the treatment of Alzheimer's disease: tangible benefits of current therapies.J Clin Psychiatry. 2006;67 Suppl 3:15-22; quiz 23. J Clin Psychiatry. 2006. PMID: 16649847 Review.
Cited by
-
Ethnoracial Differences in Lewy Body Diseases with Cognitive Impairment.J Alzheimers Dis. 2020;77(1):165-174. doi: 10.3233/JAD-200395. J Alzheimers Dis. 2020. PMID: 32804137 Free PMC article.
-
Sex Differences in the Prevalent Use of Oral Formulations of Cholinesterase Inhibitors in Older Adults with Dementia.Drugs Aging. 2019 Sep;36(9):875-884. doi: 10.1007/s40266-019-00690-9. Drugs Aging. 2019. PMID: 31309528
-
Concentration-Dependent Activity of Hydromethylthionine on Cognitive Decline and Brain Atrophy in Mild to Moderate Alzheimer's Disease.J Alzheimers Dis. 2019;72(3):931-946. doi: 10.3233/JAD-190772. J Alzheimers Dis. 2019. PMID: 31658058 Free PMC article. Clinical Trial.
-
Alzheimer's disease medication use and adherence patterns by race and ethnicity.Alzheimers Dement. 2023 Apr;19(4):1184-1193. doi: 10.1002/alz.12753. Epub 2022 Aug 8. Alzheimers Dement. 2023. PMID: 35939325 Free PMC article.
-
Aortic valve replacement among patients with Alzheimer's disease and related dementias.J Am Geriatr Soc. 2021 Dec;69(12):3468-3475. doi: 10.1111/jgs.17432. Epub 2021 Sep 8. J Am Geriatr Soc. 2021. PMID: 34498253 Free PMC article.
References
-
- Prince MJ, Bryce R, Albanese E, et al. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimers Dement. 2013;9(1):63–75. - PubMed
-
- Wimo A, Jönsson L, Bond J, et al. The worldwide economic impact of dementia 2010. Alzheimers Dement. 2013;9(1):1–11. e3. - PubMed
-
- National Alzheimer's Project Act. USA: 2011. Public Law 111 -375-Jan 4 2011.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
