

Optimal timing of antiretroviral treatment initiation in HIV-positive children and adolescents: a multiregional analysis from Southern Africa, West Africa and Europe
- PMID: 27342220
- PMCID: PMC5837574
- DOI: 10.1093/ije/dyw097
Optimal timing of antiretroviral treatment initiation in HIV-positive children and adolescents: a multiregional analysis from Southern Africa, West Africa and Europe
Abstract
Background: There is limited knowledge about the optimal timing of antiretroviral treatment initiation in older children and adolescents.
Methods: A total of 20 576 antiretroviral treatment (ART)-naïve patients, aged 1-16 years at enrolment, from 19 cohorts in Europe, Southern Africa and West Africa, were included. We compared mortality and growth outcomes for different ART initiation criteria, aligned with previous and recent World Health Organization criteria, for 5 years of follow-up, adjusting for all measured baseline and time-dependent confounders using the g-formula.
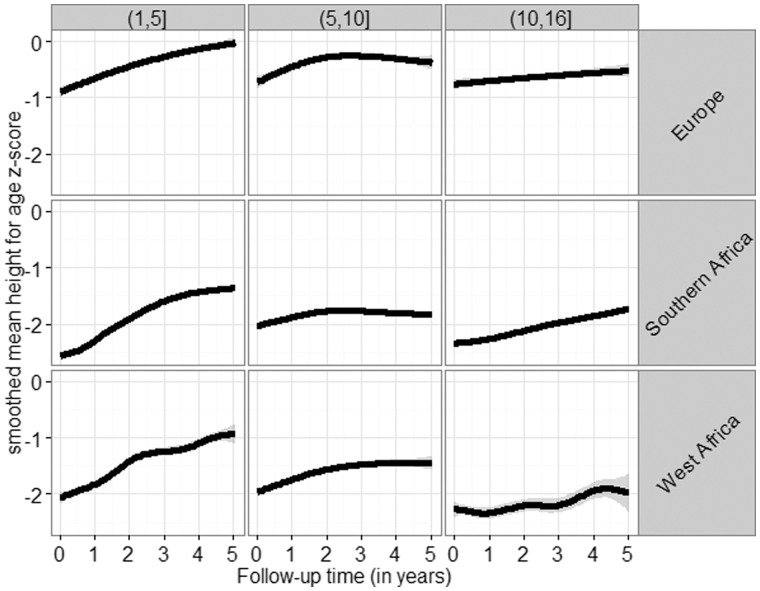
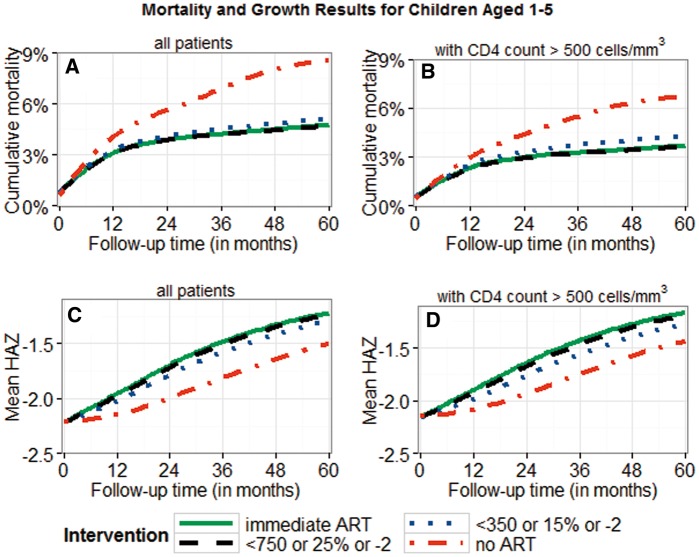
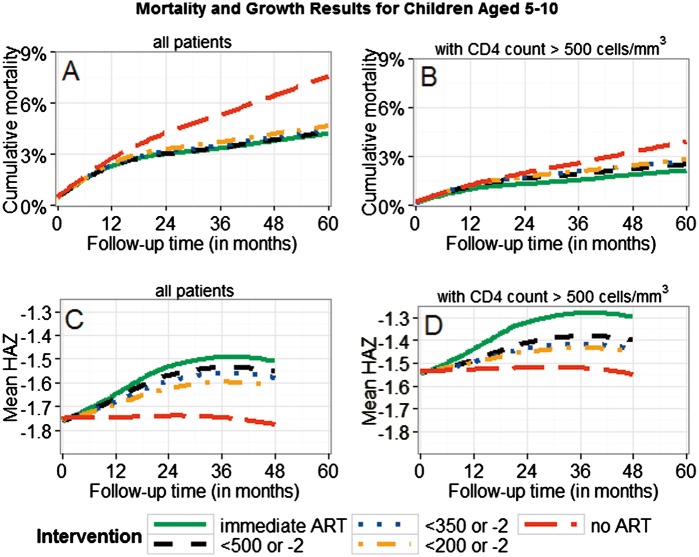
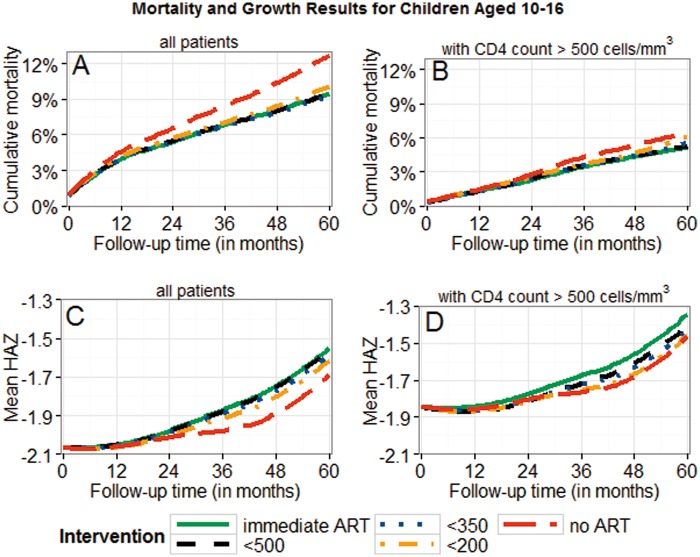
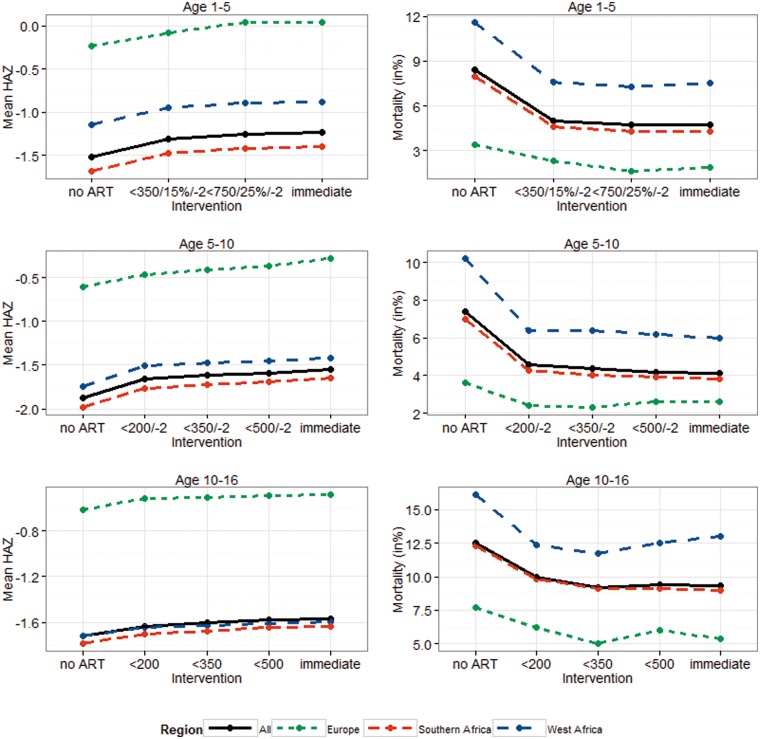
Results: Median (1st;3rd percentile) CD4 count at baseline was 676 cells/mm 3 (394; 1037) (children aged ≥ 1 and < 5 years), 373 (172; 630) (≥ 5 and < 10 years) and 238 (88; 425) (≥ 10 and < 16 years). There was a general trend towards lower mortality and better growth with earlier treatment initiation. In children < 10 years old at enrolment, by 5 years of follow-up there was lower mortality and a higher mean height-for-age z-score with immediate ART initiation versus delaying until CD4 count < 350 cells/mm 3 (or CD4% < 15% or weight-for-age z-score < -2) with absolute differences in mortality and height-for-age z-score of 0.3% (95% confidence interval: 0.1%; 0.6%) and -0.08 (-0.09; -0.06) (≥ 1 and < 5 years), and 0.3% (0.04%; 0.5%) and -0.07 (-0.08; -0.05) (≥ 5 and < 10 years). In those aged > 10 years at enrolment we did not find any difference in mortality or growth with immediate ART initiation, with estimated differences of -0.1% (-0.2%; 0.6%) and -0.03 (-0.05; 0.00), respectively. Growth differences in children aged < 10 years persisted for treatment thresholds using higher CD4 values. Regular follow-up led to better height and mortality outcomes.
Conclusions: Immediate ART is associated with lower mortality and better growth for up to 5 years in children < 10 years old. Our results on adolescents were inconclusive.
Keywords: Antiretroviral treatment; causal inference; g-formula; paediatrics.
© The Author 2016; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association
Figures
References
-
- WHO. Antiretroviral Therapy of HIV Infection in Infants and Children. 2006. http://www.who.int/hiv/pub/guidelines/en/
-
- WHO. Antiretroviral Therapy for HIV Infection in Adults and Adolescents. 2006. http://www.who.int/hiv/pub/guidelines/en/
-
- Puthanakit T, Bunupuradah T.. Early versus deferred antiretroviral therapy in children in low-income and middle-income countries. Curr Opin HIV/AIDS 2010;5:12-17. - PubMed
-
- Schomaker M. Implications of causal modelling studies on the question of when to start antiretroviral treatment in young children. SACEMA Q 2014. http://sacemaquarterly.com/wp-content/uploads/2014/11/Michael_Implicatio...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
