

Local resection of the stomach for gastric cancer
- PMID: 27342746
- PMCID: PMC5406487
- DOI: 10.1007/s00595-016-1371-z
Local resection of the stomach for gastric cancer
Abstract
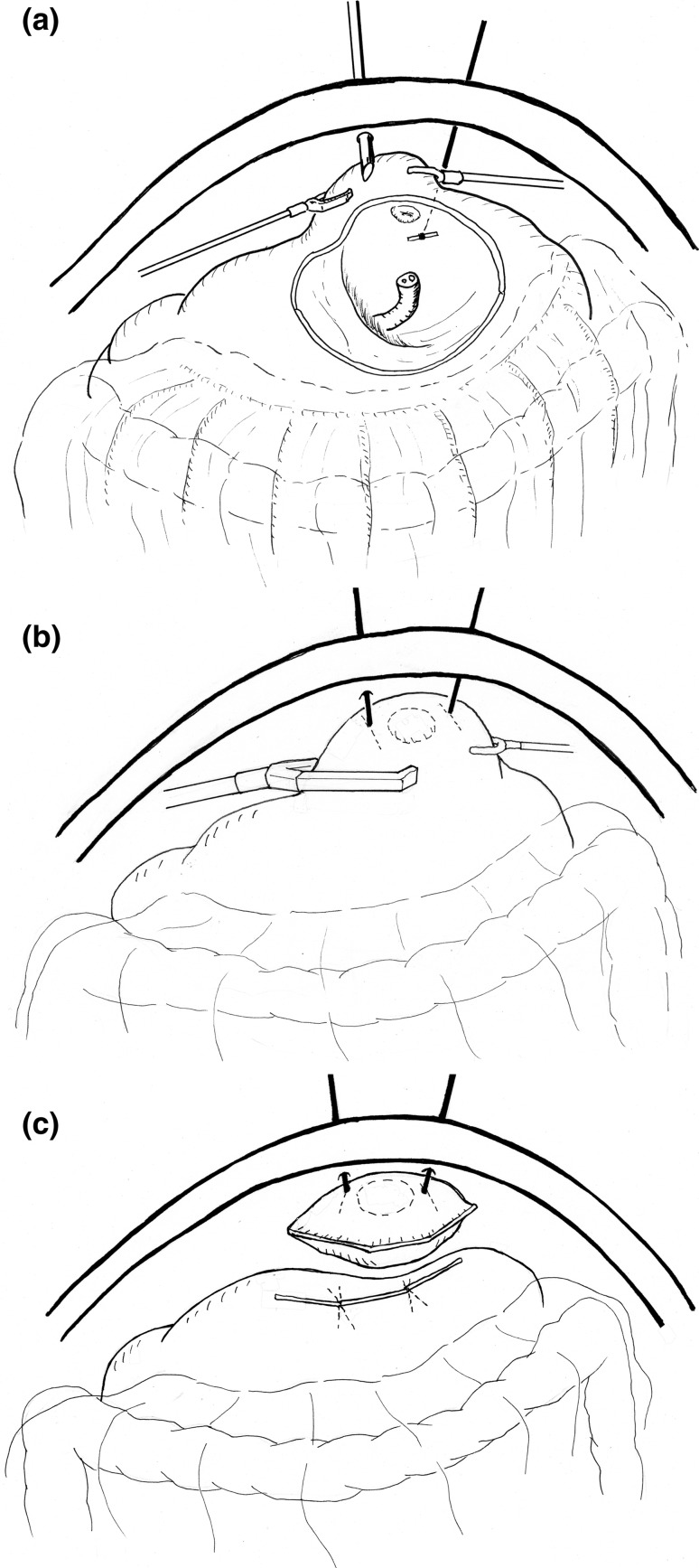
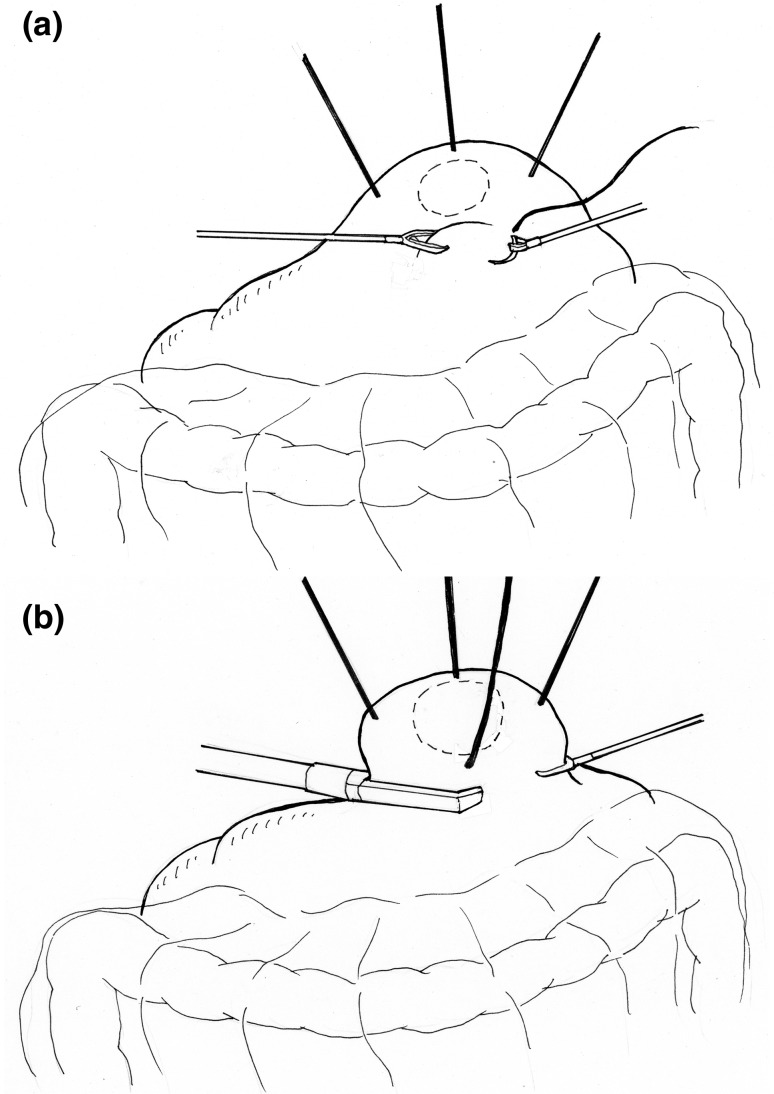
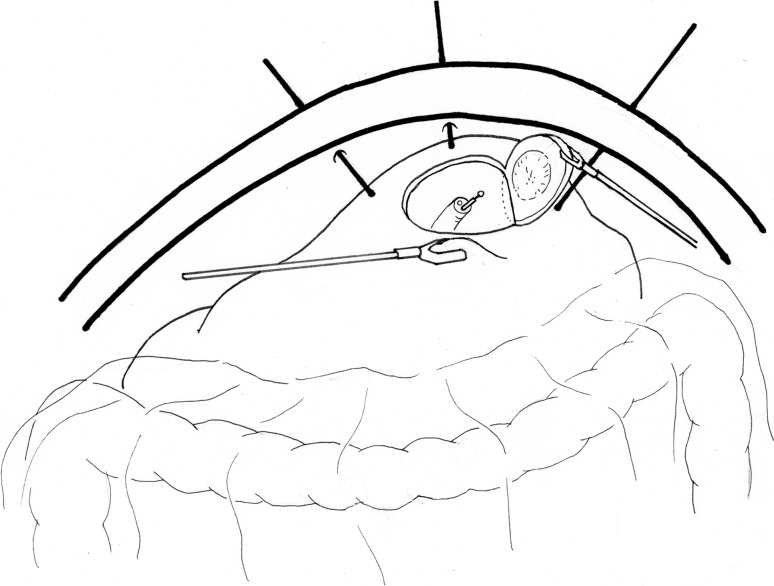
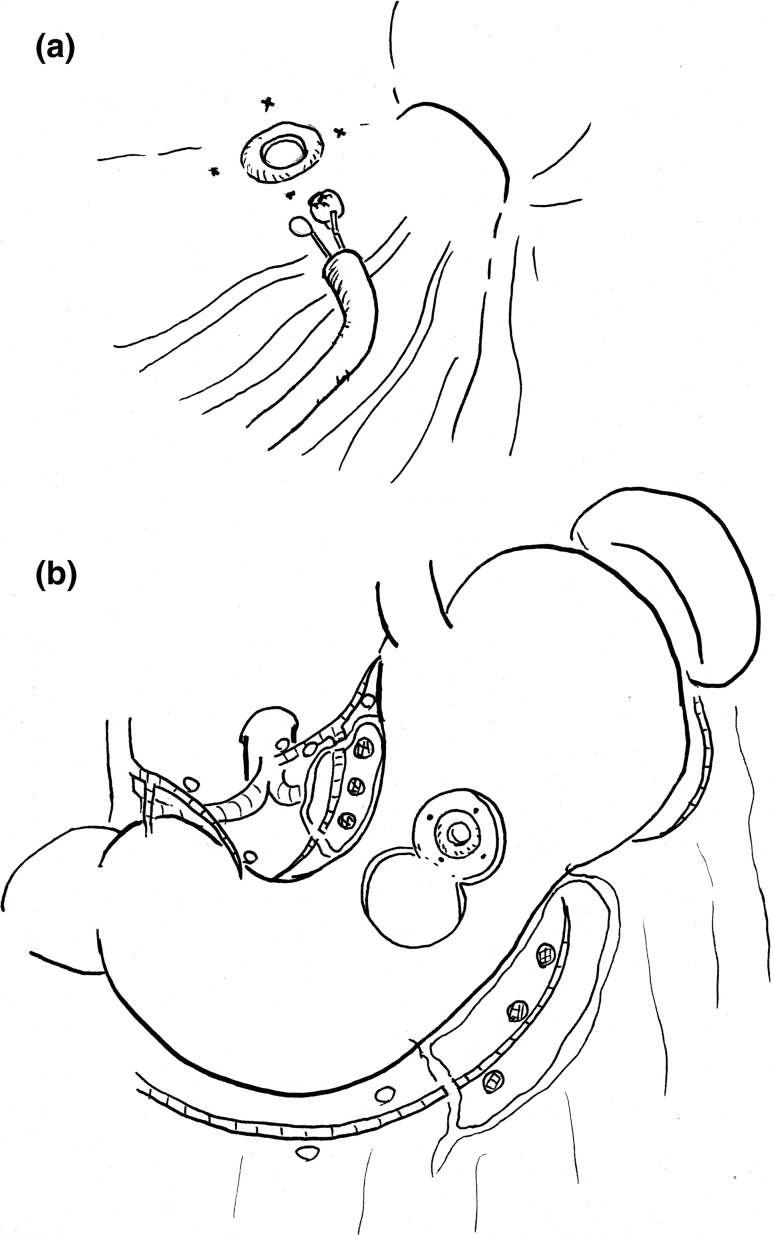
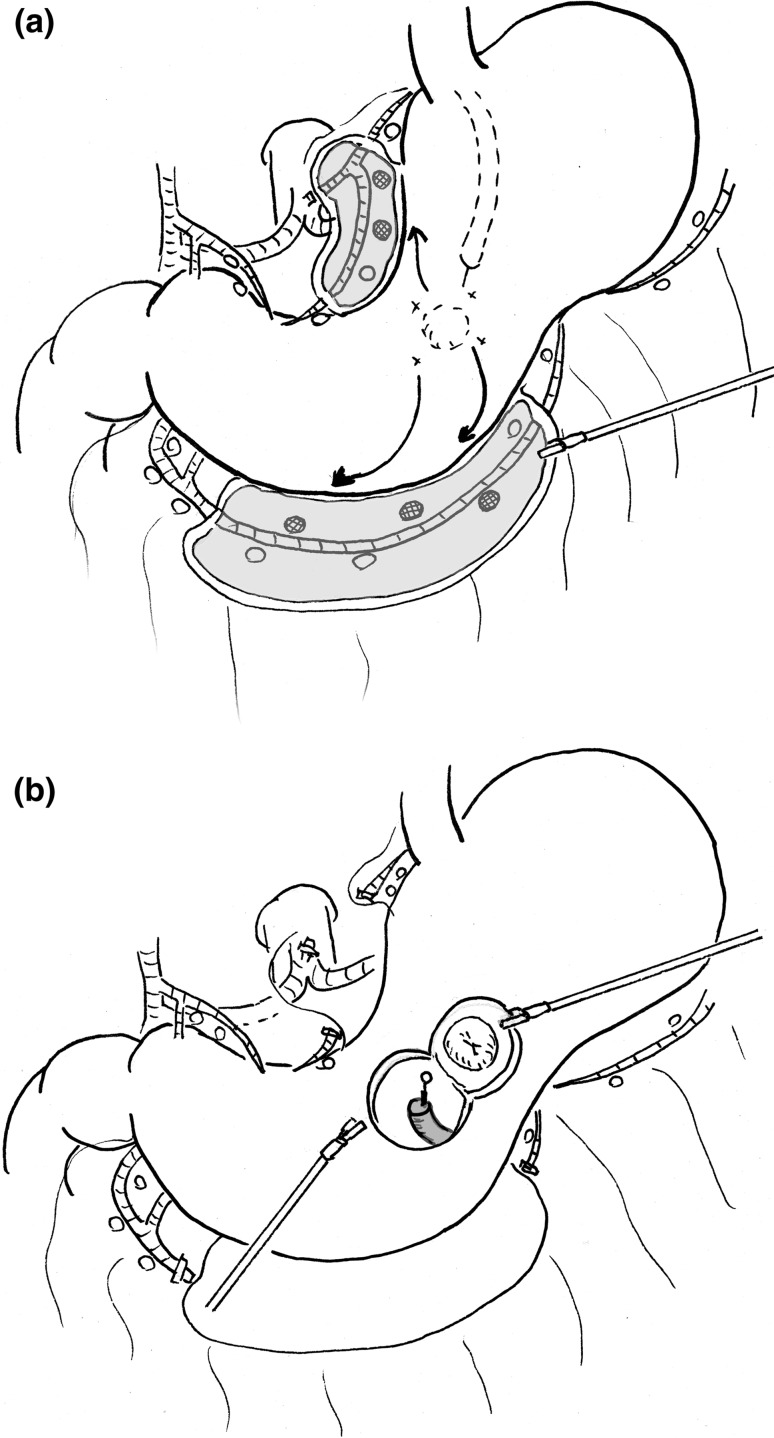
The local resection of the stomach is an ideal method for preventing postoperative symptoms. There are various procedures for performing local resection, such as the laparoscopic lesion lifting method, non-touch lesion lifting method, endoscopic full-thickness resection, and laparoscopic endoscopic cooperative surgery. After the invention and widespread use of endoscopic submucosal dissection, local resection has become outdated as a curative surgical technique for gastric cancer. Nevertheless, local resection of the stomach in the treatment of gastric cancer in now expected to make a comeback with the clinical use of sentinel node navigation surgery. However, there are many issues associated with local resection for gastric cancer, other than the normal indications. These include gastric deformation, functional impairment, ensuring a safe surgical margin, the possibility of inducing peritoneal dissemination, and the associated increase in the risk of metachronous gastric cancer. In view of these issues, there is a tendency to regard local resection as an investigative treatment, to be applied only in carefully selected cases. The ideal model for local resection of the stomach for gastric cancer would be a combination of endoscopic full-thickness resection of the stomach using an ESD device and hand sutured closure using a laparoscope or a surgical robot, for achieving both oncological safety and preserved functions.
Keywords: Gastric cancer; Laparoscopic endoscopic cooperative surgery; Local resection; Sentinel node.
Figures
References
-
- Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC cancer staging manual, 7th edn. New York, Springer; 2010. p. 3–14.
-
- Nakada K, Ikeda M, Takahashi M, Kinami S, Yoshida M, Uenosono Y, et al. Characteristics and clinical relevance of postgastrectomy syndrome assessment scale (PGSAS)-45: newly developed integrated questionnaires for assessment of living status and quality of life in postgastrectomy patients. Gastric Cancer. 2015;18:147–158. doi: 10.1007/s10120-014-0344-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
