

Cardiovascular Late Effects and Exercise Treatment in Breast Cancer: Current Evidence and Future Directions
- PMID: 27343744
- PMCID: PMC5512173
- DOI: 10.1016/j.cjca.2016.03.014
Cardiovascular Late Effects and Exercise Treatment in Breast Cancer: Current Evidence and Future Directions
Abstract
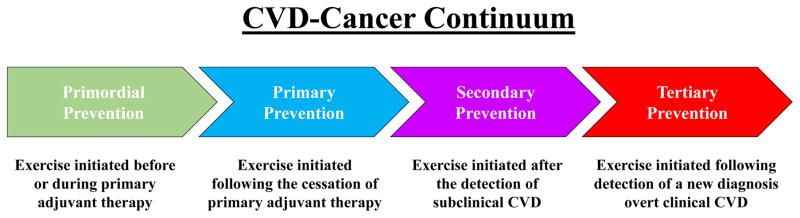
Advances in detection and supportive care strategies have led to improvements in cancer-specific and overall survival after a diagnosis of early-stage breast cancer. These improvements, however, are associated with an increase in competing forms of morbidity and mortality, particularly cardiovascular disease (CVD). Indeed, in certain subpopulations of patients, CVD is the leading cause of mortality after early breast cancer, and these women also have an increased risk of CVD-specific morbidity, including an elevated incidence of coronary artery disease and heart failure compared with their sex- and age-matched counterparts. Exercise treatment is established as the cornerstone of primary and secondary prevention of CVD in multiple clinical populations. The potential benefits of exercise treatment to modulate CVD or CVD risk factors before, immediately after, or in the months/years after adjuvant therapy for early-stage breast cancer have received limited attention. We discuss the risk and extent of CVD in patients with breast cancer, review the pathogenesis of CVD, and highlight existing evidence from select clinical trials investigating the efficacy of structured exercise treatment across the CVD continuum in early breast cancer.
Copyright © 2016 Canadian Cardiovascular Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Cardiovascular disease following hematopoietic stem cell transplantation: Pathogenesis, detection, and the cardioprotective role of aerobic training.Crit Rev Oncol Hematol. 2016 Feb;98:222-34. doi: 10.1016/j.critrevonc.2015.11.007. Epub 2015 Nov 17. Crit Rev Oncol Hematol. 2016. PMID: 26643524 Free PMC article. Review.
-
Curing breast cancer and killing the heart: A novel model to explain elevated cardiovascular disease and mortality risk among women with early stage breast cancer.Prog Cardiovasc Dis. 2019 Mar-Apr;62(2):116-126. doi: 10.1016/j.pcad.2019.02.002. Epub 2019 Feb 22. Prog Cardiovasc Dis. 2019. PMID: 30797800 Review.
-
Personalizing cardiovascular disease prevention among breast cancer survivors.Curr Opin Cardiol. 2012 Sep;27(5):515-24. doi: 10.1097/HCO.0b013e3283570040. Curr Opin Cardiol. 2012. PMID: 22874128 Review.
-
Exercise therapy as treatment for cardiovascular and oncologic disease after a diagnosis of early-stage cancer.Semin Oncol. 2013 Apr;40(2):218-28. doi: 10.1053/j.seminoncol.2013.01.001. Semin Oncol. 2013. PMID: 23540747 Review.
-
Assessment of risk factors for mortality in patients with cardiovascular disease and a history of treatment for malignancy.Kardiol Pol. 2015;73(9):730-9. doi: 10.5603/KP.a2015.0071. Kardiol Pol. 2015. PMID: 26390319
Cited by
-
Adenosine 5'-Triphosphate Metabolism in Red Blood Cells as a Potential Biomarker for Post-Exercise Hypotension and a Drug Target for Cardiovascular Protection.Metabolites. 2018 May 2;8(2):30. doi: 10.3390/metabo8020030. Metabolites. 2018. PMID: 29724022 Free PMC article. Review.
-
Cardio-Oncology - A new subspecialty with collaboration at its heart.Indian Heart J. 2017 Jul-Aug;69(4):556-562. doi: 10.1016/j.ihj.2017.05.006. Epub 2017 May 27. Indian Heart J. 2017. PMID: 28822531 Free PMC article. Review.
-
Oncology and Cardiac Rehabilitation: An Underrated Relationship.J Clin Med. 2020 Jun 10;9(6):1810. doi: 10.3390/jcm9061810. J Clin Med. 2020. PMID: 32532011 Free PMC article. Review.
-
Adiposity, post-diagnosis weight change, and risk of cardiovascular events among early-stage breast cancer survivors.Breast Cancer Res Treat. 2017 Apr;162(3):549-557. doi: 10.1007/s10549-017-4133-8. Epub 2017 Feb 7. Breast Cancer Res Treat. 2017. PMID: 28176174 Free PMC article.
-
Young Adult Cancer Survivorship: Recommendations for Patient Follow-up, Exercise Therapy, and Research.JNCI Cancer Spectr. 2020 Oct 28;5(1):pkaa099. doi: 10.1093/jncics/pkaa099. eCollection 2021 Feb. JNCI Cancer Spectr. 2020. PMID: 33681702 Free PMC article. Review.
References
-
- Jatoi I, Chen BE, Anderson WF, Rosenberg PS. Breast cancer mortality trends in the United States according to estrogen receptor status and age at diagnosis. J Clin Oncol. 2007;25(13):1683–1690. - PubMed
-
- DeSantis C, Jemal A, Ward E, Thun MJ. Temporal trends in breast cancer mortality by state and race. Cancer causes & control : CCC. 2008;19(5):537–545. - PubMed
-
- Hooning MJ, Aleman BM, van Rosmalen AJ, Kuenen MA, Klijn JG, van Leeuwen FE. Cause-specific mortality in long-term survivors of breast cancer: A 25-year follow-up study. Int J Radiat Oncol Biol Phys. 2006;64(4):1081–1091. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
