

Localization of the Lateral Retinacular Nerve for Diagnostic and Therapeutic Nerve Block for Lateral Knee Pain: A Cadaveric Study
- PMID: 27346091
- PMCID: PMC5182177
- DOI: 10.1016/j.pmrj.2016.06.017
Localization of the Lateral Retinacular Nerve for Diagnostic and Therapeutic Nerve Block for Lateral Knee Pain: A Cadaveric Study
Abstract
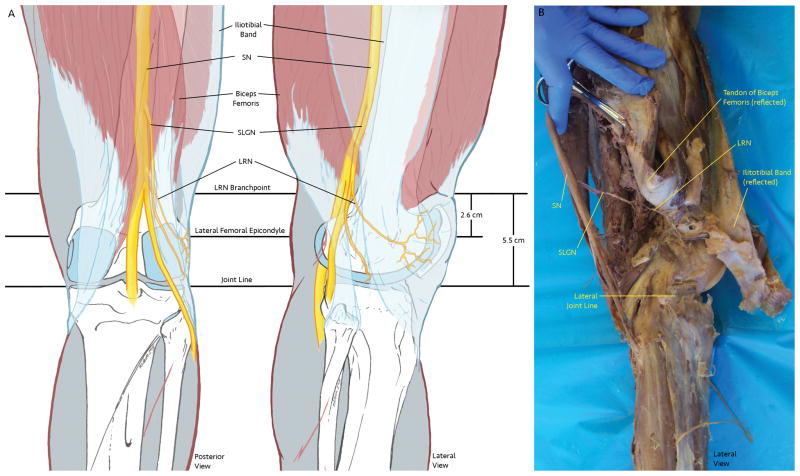
Background: The lateral retinacular nerve (LRN) is a branch of the superior lateral genicular nerve (SLGN) and is believed to contribute to anterolateral knee pain. The precise anatomical pathway of the LRN, however, has not been demonstrated as it relates to the performance of targeted nerve block procedures.
Objective: To describe the anatomical landmarks for localization of the LRN to facilitate diagnostic and therapeutic nerve blocks in the treatment of chronic anterolateral knee pain.
Design: Descriptive study.
Setting: Anatomy dissection laboratory in an academic institution.
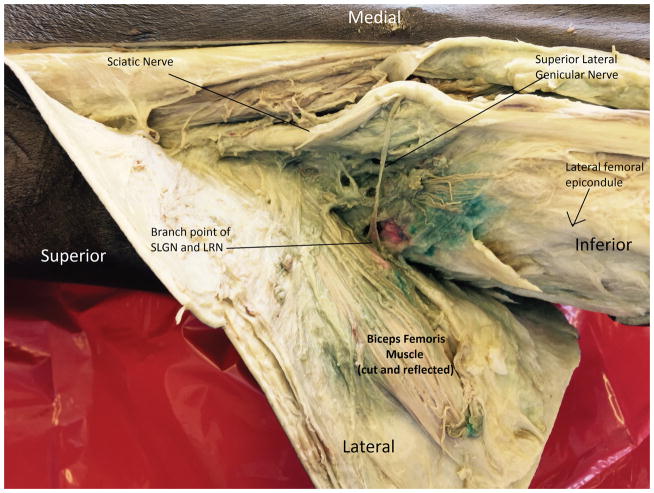
Methods: Twenty lower extremities were dissected in 12 cadavers. The sciatic nerve was identified, and its branch to the posterior aspect of the knee, the SLGN, was dissected. The SLGN dissection was continued distally to identify its first branch, the LRN. Two measurements were taken from the branch point on the lateral knee deep to the distal biceps tendon in alignment with the fibular head. A validation study completed in 4 knees was performed as follows: 1 mL of colored dye was injected at the first and second measurements. The cadaveric knee was then dissected to assess the accuracy.
Main outcome measurements: Localization of the branch point of the LRN from the SLGN via dissection and then direct assessment of injected dye at the measurement points via dissection.
Results: The branch point of the LRN from the SLGN was, on average, 5.5 ± 0.66 cm (with a range of 4.5-7.0 cm) proximal to the lateral tibiofemoral joint line in line with the head of the fibula and 2.6 ± 0.62 cm (2.0-4.5 cm) proximal to the tip of the lateral femoral epicondyle. On assessment of the 2 measurements, the measurement 5.5 cm proximal to the lateral joint line accurately targeted the branch point in 100% (4/4) of the knees, whereas the measurement 2.6 cm proximal the tip of the lateral femoral epicondyle accurately targeted the branch point in 75% (3/4) of the knees.
Conclusion: The results of this study provide 2 dependable landmarks and a description of the path of the LRN, making it possible to accurately target the LRN to diagnose and alleviate lateral knee pain.
Copyright © 2017 American Academy of Physical Medicine and Rehabilitation. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Distribution of sensory nerves supplying the knee joint capsule and implications for genicular blockade and radiofrequency ablation: an anatomical study.Surg Radiol Anat. 2019 Dec;41(12):1461-1471. doi: 10.1007/s00276-019-02291-y. Epub 2019 Jul 23. Surg Radiol Anat. 2019. PMID: 31338537
-
Accuracy of Ultrasound-Guided Genicular Nerve Block: A Cadaveric Study.Pain Physician. 2015 Sep-Oct;18(5):E899-904. Pain Physician. 2015. PMID: 26431143
-
Genicular Nerve Anatomy and Its Implication for New Procedural Approaches for Knee Joint Denervation: A Cadaveric Study.Pain Med. 2022 Jan 3;23(1):144-151. doi: 10.1093/pm/pnab238. Pain Med. 2022. PMID: 34625814
-
Innervation of the Anterior Capsule of the Human Knee: Implications for Radiofrequency Ablation.Reg Anesth Pain Med. 2015 Jul-Aug;40(4):363-8. doi: 10.1097/AAP.0000000000000269. Reg Anesth Pain Med. 2015. PMID: 26066383 Review.
-
The surgical anatomy of the infrapatellar branch of the saphenous nerve in relation to incisions for anteromedial knee surgery.J Bone Joint Surg Am. 2013 Dec 4;95(23):2119-25. doi: 10.2106/JBJS.L.01297. J Bone Joint Surg Am. 2013. PMID: 24306699 Review.
Cited by
-
Surgeon-Administered Anterolateral Geniculate Nerve Block as an Adjunct to Regional Anesthetic for Pain Management Following Anterior Cruciate Ligament Reconstruction.Arthrosc Tech. 2022 Jan 20;11(1):e1-e6. doi: 10.1016/j.eats.2021.08.034. eCollection 2022 Jan. Arthrosc Tech. 2022. PMID: 35127422 Free PMC article.
-
Distribution of sensory nerves supplying the knee joint capsule and implications for genicular blockade and radiofrequency ablation: an anatomical study.Surg Radiol Anat. 2019 Dec;41(12):1461-1471. doi: 10.1007/s00276-019-02291-y. Epub 2019 Jul 23. Surg Radiol Anat. 2019. PMID: 31338537
-
Efficacy of Genicular Nerve Block in Patients with Osteoarthritis: A Comparative Study with and without Fluoroscopy Assistance.Rev Bras Ortop (Sao Paulo). 2024 Dec 21;59(6):e876-e882. doi: 10.1055/s-0044-1793825. eCollection 2024 Dec. Rev Bras Ortop (Sao Paulo). 2024. PMID: 39711628 Free PMC article.
-
Comparing the effectiveness of ultrasound guided versus blind genicular nerve block on pain, muscle strength with isokinetic device, physical function and quality of life in chronic knee osteoarthritis: a prospective randomized controlled study.Korean J Pain. 2020 Jul 1;33(3):258-266. doi: 10.3344/kjp.2020.33.3.258. Korean J Pain. 2020. PMID: 32606270 Free PMC article.
-
Efficacy and Temporal Dynamics of Genicular Nerve Block in Primary and Secondary Knee Osteoarthritis for Pain and Function: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Pain Res. 2025 Jun 17;18:3037-3048. doi: 10.2147/JPR.S518315. eCollection 2025. J Pain Res. 2025. PMID: 40546829 Free PMC article. Review.
References
-
- Collado H, Fredericson M. Patellofemoral pain syndrome. Clinics in sports medicine. 2010 Jul;29(3):379–398. - PubMed
-
- Fulkerson JP. Histologic evidence of retinacular nerve injury associated with patellofemoral malalignment. Clinical orthopaedics and related research. 1985;(197):196–205. - PubMed
-
- Fulkerson JP. Diagnosis and Treatment of Patients with Patellofemoral Pain. The American journal of sports medicine. 2002;30(3) - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
