

Liver resection for perihilar cholangiocarcinoma - why left is sometimes right
- PMID: 27346137
- PMCID: PMC4925796
- DOI: 10.1016/j.hpb.2016.05.002
Liver resection for perihilar cholangiocarcinoma - why left is sometimes right
Abstract
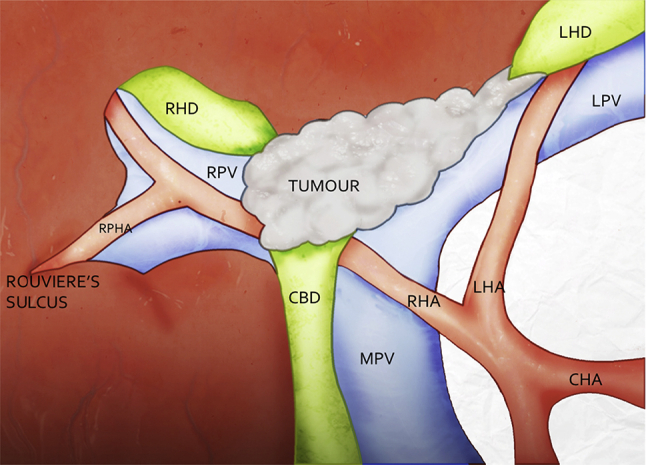
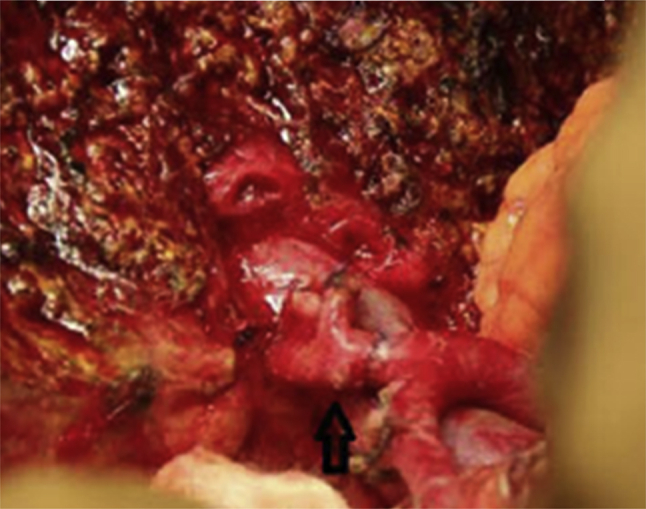
Introduction: Left-sided liver resection (LLR) for perihilar cholangiocarcinoma (PHC) may require right hepatic artery (RHA) resection and reconstruction because of its intimate relationship with the biliary confluence. Consequently right-sided resections (RLR) are preferred for Bismuth-Corlette IIIb tumours, and resections avoided in Bismuth-Corlette IV tumours with left lobar atrophy when the RHA is involved by tumour.
Methods: A retrospective analysis of patients with PHC who presented between December 2009 and June 2015.
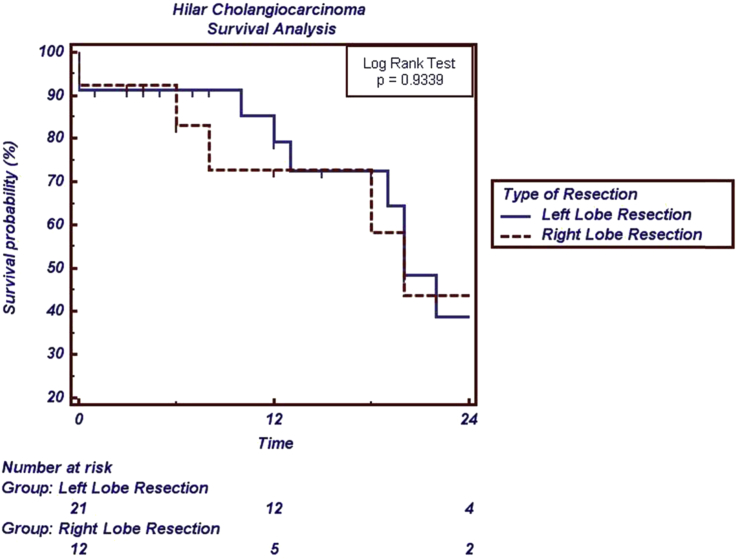
Results: Thirty-six patients underwent resection for PHC (23 LLR, 13 RLR). The number of Bismuth-Corlette IV patients undergoing LLR was significantly greater than those undergoing RLR (8/23 vs 0/13, p = 0.032). The need for arterial reconstruction (AR) was significantly greater during LLR than RLR (10/23 vs 0/13, p = 0.006). Postoperative liver dysfunction was greater after RLR (5/13 vs 0/23, p = 0.003), and hospital stay was shorter after LLR (10 vs 15 days, p = 0.013).
Conclusions: Safe AR increases the ability to perform potentially curative LLR for PHC. This improves the resectability rate for PHC, particularly for Bismuth-Corlette Type IV tumours. The larger liver remnant after LLR results in less postoperative liver dysfunction and shorter hospital stay without increased operating time, blood loss or morbidity.
Copyright © 2016 International Hepato-Pancreato-Biliary Association Inc. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Furusawa N., Kobayashi A., Yokoyama T., Shimizu A., Motoyama H., Miyagawa S. Surgical treatment of 144 cases of hilar cholangiocarcinoma without liver-related mortality. World J Surg. 2014;38:1164–1176. - PubMed
-
- Govil S., Reddy M.S., Rela M. Surgical resection techniques for locally advanced hilar cholangiocarcinoma. Langenbecks Arch Surg. 2014;399:707–716. - PubMed
-
- Ratti F., Cipriani F., Piozzi G., Catena M., Paganelli M., Aldrighetti L. Comparative analysis of left- versus right-sided resection in Klatskin tumor surgery: can lesion side be considered a prognostic factor? J Gastrointest Surg. 2015;19:1324–1333. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
