

The Role of Neuroimaging Techniques in Establishing Diagnosis, Prognosis and Therapy in Disorders of Consciousness
- PMID: 27347265
- PMCID: PMC4894918
- DOI: 10.2174/1874440001610010052
The Role of Neuroimaging Techniques in Establishing Diagnosis, Prognosis and Therapy in Disorders of Consciousness
Abstract
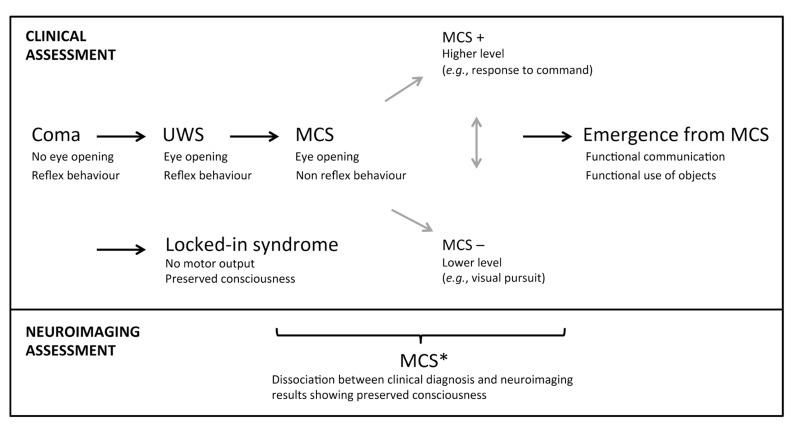
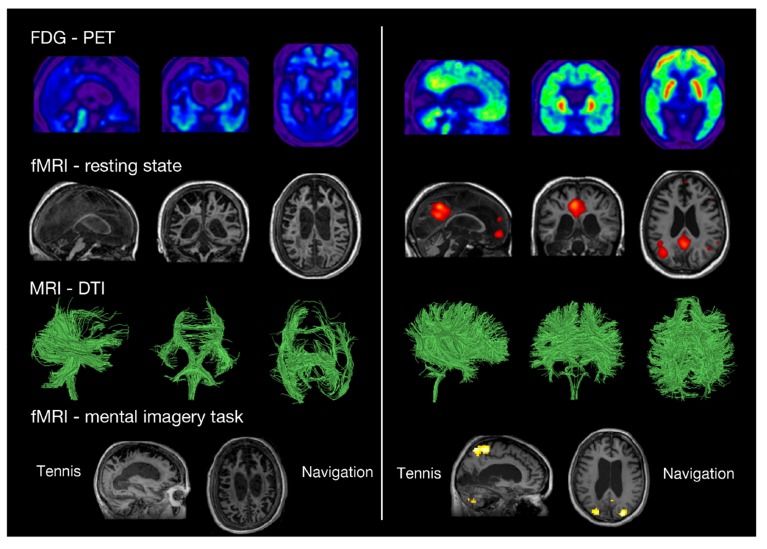
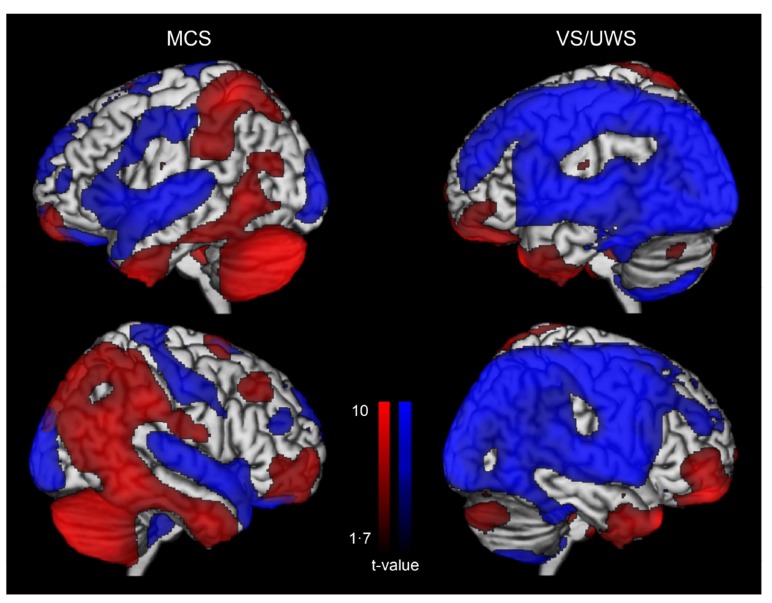
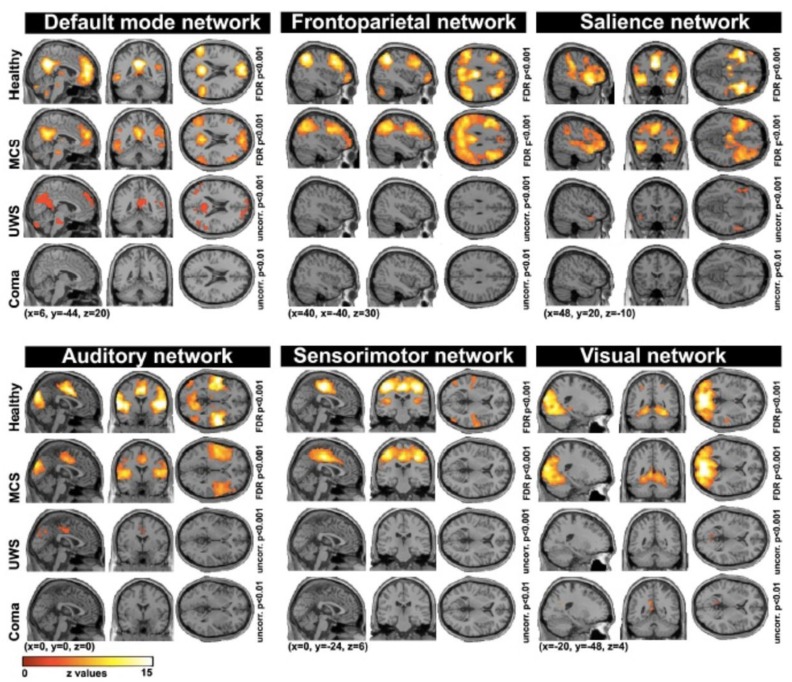
Non-communicative brain damaged patients raise important clinical and scientific issues. Here, we review three major pathological disorders of consciousness: coma, the unresponsive wakefulness syndrome and the minimally conscious state. A number of clinical studies highlight the difficulty in making a correct diagnosis in patients with disorders of consciousness based only on behavioral examinations. The increasing use of neuroimaging techniques allows improving clinical characterization of these patients. Recent neuroimaging studies using positron emission tomography, functional magnetic resonance imaging, electroencephalography and transcranial magnetic stimulation can help assess diagnosis, prognosis, and therapeutic treatment. These techniques, using resting state, passive and active paradigms, also highlight possible dissociations between consciousness and responsiveness, and are facilitating a more accurate understanding of brain function in this challenging population.
Keywords: Coma; EEG; PET scan; fMRI; minimally conscious state; neuroimaging; unresponsive wakefulness syndrome.
Figures
References
-
- Posner J.B., Saper C.B., Schiff N.D., Plum F. Plum and Posner's diagnosis of stupor and coma. Oxford: Oxford University Press 2007.
-
- Plum F., Posner J.B. The diagnosis of stupor and coma. Contemp. Neurol. Ser. 1972;10:1–286. - PubMed
-
- Laureys S., Celesia G.G., Cohadon F., Lavrijsen J., León-Carrión J., Sannita W.G., Sazbon L., Schmutzhard E., von Wild K.R., Zeman A., Dolce G., European Task Force on Disorders of Consciousness Unresponsive wakefulness syndrome: a new name for the vegetative state or apallic syndrome. BMC Med. 2010;8:68. doi: 10.1186/1741-7015-8-68. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources