

Regional Longitudinal Myocardial Deformation Provides Incremental Prognostic Information in Patients with ST-Segment Elevation Myocardial Infarction
- PMID: 27348525
- PMCID: PMC4922592
- DOI: 10.1371/journal.pone.0158280
Regional Longitudinal Myocardial Deformation Provides Incremental Prognostic Information in Patients with ST-Segment Elevation Myocardial Infarction
Abstract
Background: Global longitudinal systolic strain (GLS) has recently been demonstrated to be a superior prognosticator to conventional echocardiographic measures in patients after myocardial infarction (MI). The aim of this study was to evaluate the prognostic value of regional longitudinal myocardial deformation in comparison to GLS, conventional echocardiography and clinical information.
Method: In total 391 patients were admitted with ST-Segment elevation myocardial infarction (STEMI), treated with primary percutaneous coronary intervention and subsequently examined by echocardiography. All patients were examined by tissue Doppler imaging (TDI) and two-dimensional strain echocardiography (2DSE).
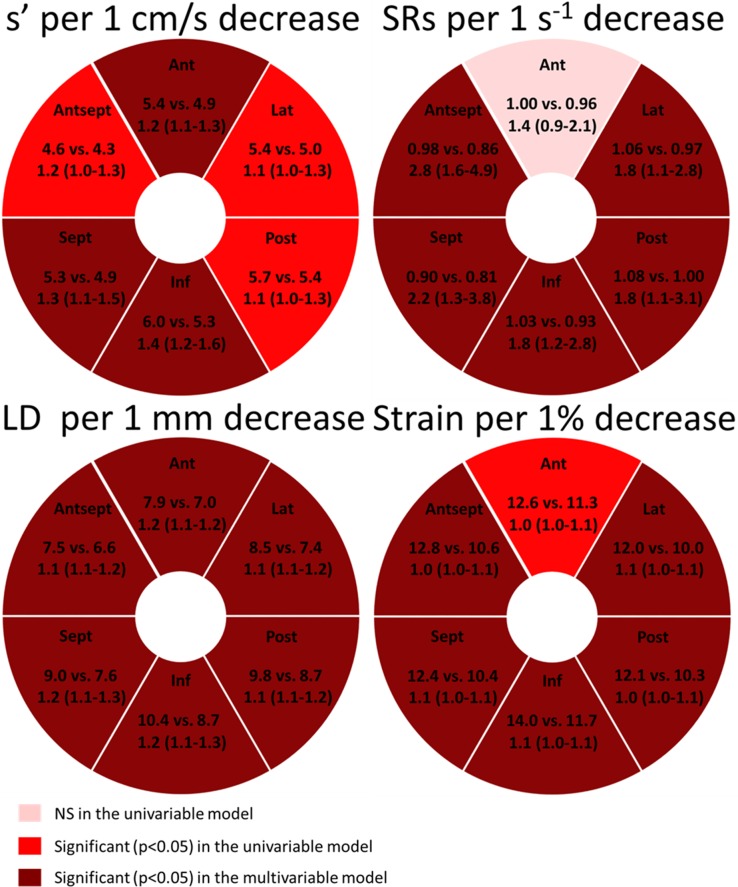
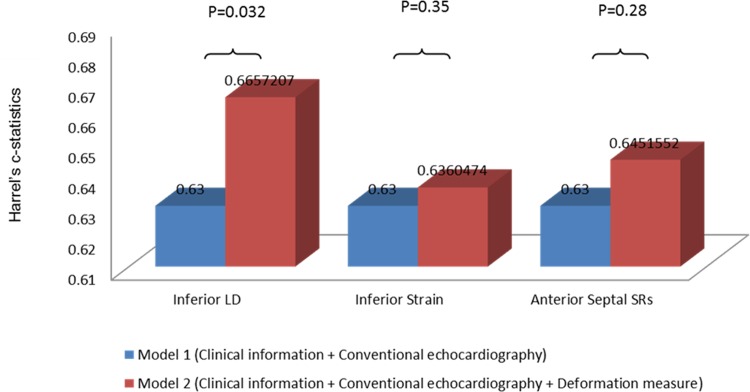
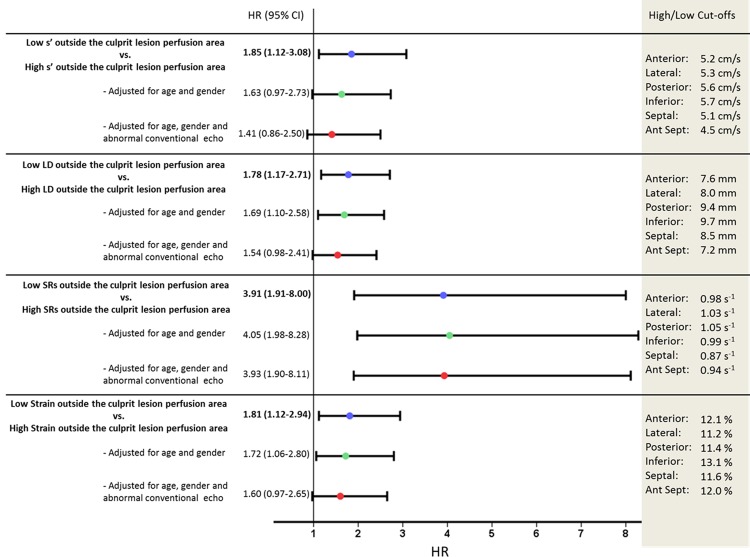
Results: During a median-follow-up of 5.3 (IQR 2.5-6.1) years the primary endpoint (death, heart failure or a new MI) was reached by 145 (38.9%) patients. After adjustment for significant confounders (including conventional echocardiographic parameters) and culprit lesion, reduced longitudinal performance in the anterior septal and inferior myocardial regions (but not GLS) remained independent predictors of the combined outcome. Furthermore, inferior myocardial longitudinal deformation provided incremental prognostic information to clinical and conventional echocardiographic information (Harrell's c-statistics: 0.63 vs. 0.67, p = 0.032). In addition, impaired longitudinal deformation outside the culprit lesion perfusion region was significantly associated with an adverse outcome (p<0.05 for all deformation parameters).
Conclusion: Regional longitudinal myocardial deformation measures, regardless if determined by TDI or 2DSE, are superior prognosticators to GLS. In addition, impaired longitudinal deformation in the inferior myocardial segment provides prognostic information over and above clinical and conventional echocardiographic risk factors. Furthermore, impaired longitudinal deformation outside the culprit lesion perfusion region seems to be a paramount marker of adverse outcome.
Conflict of interest statement
Figures
Similar articles
-
Cardiac time intervals by tissue Doppler imaging M-mode echocardiography: reproducibility, reference values, association with clinical characteristics and prognostic implications.Dan Med J. 2016 Aug;63(8):B5279. Dan Med J. 2016. PMID: 27477801
-
Prognostic value of cardiac time intervals by tissue Doppler imaging M-mode in patients with acute ST-segment-elevation myocardial infarction treated with primary percutaneous coronary intervention.Circ Cardiovasc Imaging. 2013 May 1;6(3):457-65. doi: 10.1161/CIRCIMAGING.112.000230. Epub 2013 Mar 27. Circ Cardiovasc Imaging. 2013. PMID: 23536267
-
Presence of post-systolic shortening is an independent predictor of heart failure in patients following ST-segment elevation myocardial infarction.Int J Cardiovasc Imaging. 2018 May;34(5):751-760. doi: 10.1007/s10554-017-1288-7. Epub 2017 Dec 11. Int J Cardiovasc Imaging. 2018. PMID: 29230597
-
European Association of Cardiovascular Imaging/Cardiovascular Imaging Department of the Brazilian Society of Cardiology recommendations for the use of cardiac imaging to assess and follow patients after heart transplantation.Eur Heart J Cardiovasc Imaging. 2015 Sep;16(9):919-48. doi: 10.1093/ehjci/jev139. Epub 2015 Jul 2. Eur Heart J Cardiovasc Imaging. 2015. PMID: 26139361 Review.
-
Clinical aspects of left ventricular diastolic function assessed by Doppler echocardiography following acute myocardial infarction.Dan Med Bull. 2001 Nov;48(4):199-210. Dan Med Bull. 2001. PMID: 11767125 Review.
Cited by
-
Subclinical dysfunction of remote myocardium is related to high NT-proBNP and affects global contractility at follow-up, independently of infarct area.Front Cardiovasc Med. 2022 Dec 19;9:997821. doi: 10.3389/fcvm.2022.997821. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36601063 Free PMC article.
-
Early Systolic Lengthening in Patients With ST-Segment-Elevation Myocardial Infarction: A Novel Predictor of Cardiovascular Events.J Am Heart Assoc. 2020 Feb 4;9(3):e013835. doi: 10.1161/JAHA.119.013835. Epub 2020 Jan 24. J Am Heart Assoc. 2020. PMID: 31973603 Free PMC article.
-
Anterior STEMI associated with decreased strain in remote cardiac myocardium.Int J Cardiovasc Imaging. 2022 Feb;38(2):375-387. doi: 10.1007/s10554-021-02391-0. Epub 2021 Sep 5. Int J Cardiovasc Imaging. 2022. PMID: 34482507 Free PMC article. Clinical Trial.
-
Prognostic value of left ventricular mitral annular longitudinal displacement obtained by tissue Doppler imaging in patients with heart failure with reduced ejection fraction.Open Heart. 2021 Jan;8(1):e001494. doi: 10.1136/openhrt-2020-001494. Open Heart. 2021. PMID: 33495381 Free PMC article.
-
Association between left ventricular systolic function parameters and myocardial injury, organ failure and mortality in patients with septic shock.Ann Intensive Care. 2024 Jan 18;14(1):12. doi: 10.1186/s13613-023-01235-5. Ann Intensive Care. 2024. PMID: 38236316 Free PMC article.
References
-
- Schmidt M, Jacobsen JB, Lash TL, Bøtker HE, Sørensen HT. 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ. 2012;344: e356 10.1136/bmj.e356 - DOI - PMC - PubMed
-
- White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation. 1987;76: 44–51. - PubMed
-
- St John Sutton M, Pfeffer MA, Plappert T, Rouleau JL, Moyé LA, Dagenais GR, et al. Quantitative two-dimensional echocardiographic measurements are major predictors of adverse cardiovascular events after acute myocardial infarction. The protective effects of captopril. Circulation. 1994;89: 68–75. - PubMed
-
- Volpi A, De Vita C, Franzosi MG, Geraci E, Maggioni AP, Mauri F, et al. Determinants of 6-month mortality in survivors of myocardial infarction after thrombolysis. Results of the GISSI-2 data base. The Ad hoc Working Group of the Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico (GISSI)-2 Data Base. Circulation. 1993;88: 416–429. - PubMed
-
- Thune JJ, Køber L, Pfeffer MA, Skali H, Anavekar NS, Bourgoun M, et al. Comparison of regional versus global assessment of left ventricular function in patients with left ventricular dysfunction, heart failure, or both after myocardial infarction: the valsartan in acute myocardial infarction echocardiographic study. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr. 2006;19: 1462–1465. 10.1016/j.echo.2006.05.028 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
