

Pegylated Interferon α-2a Triggers NK-Cell Functionality and Specific T-Cell Responses in Patients with Chronic HBV Infection without HBsAg Seroconversion
- PMID: 27348813
- PMCID: PMC4922676
- DOI: 10.1371/journal.pone.0158297
Pegylated Interferon α-2a Triggers NK-Cell Functionality and Specific T-Cell Responses in Patients with Chronic HBV Infection without HBsAg Seroconversion
Abstract
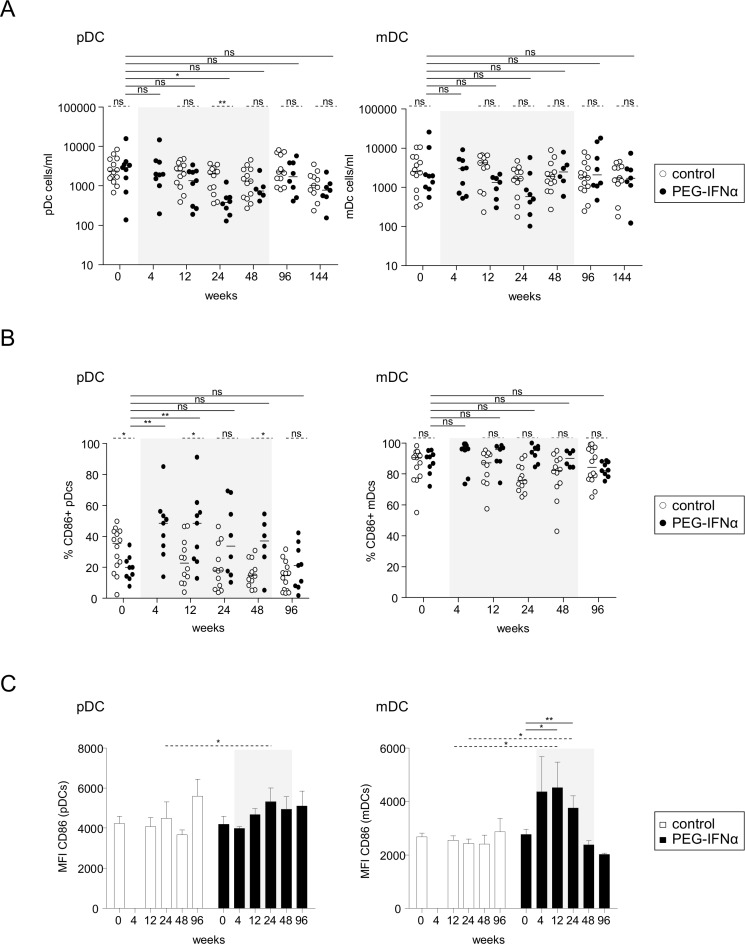
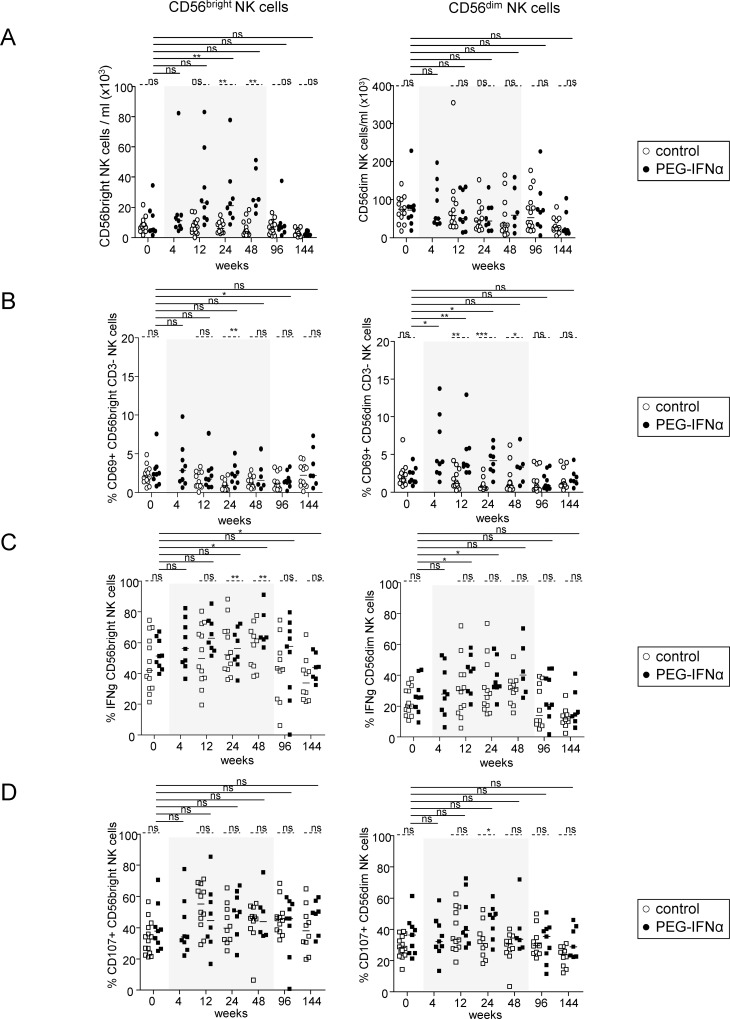
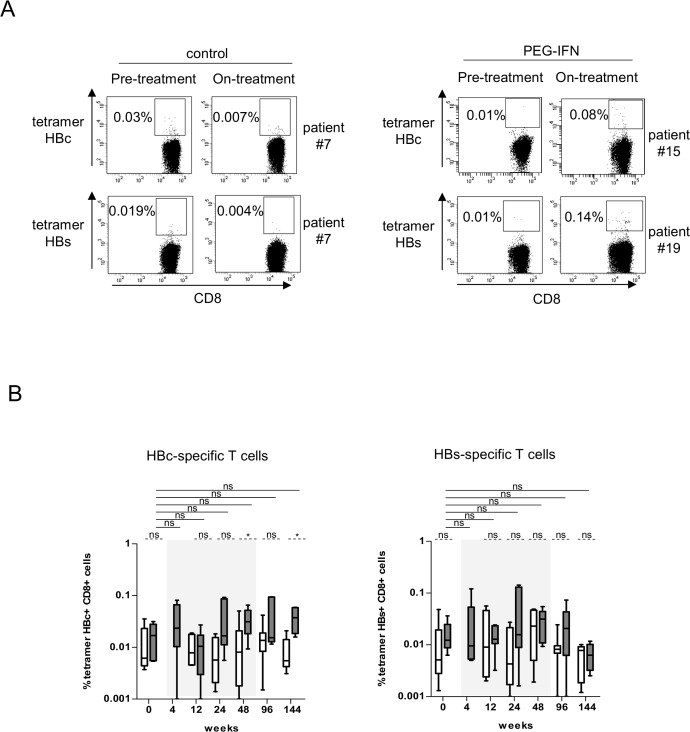
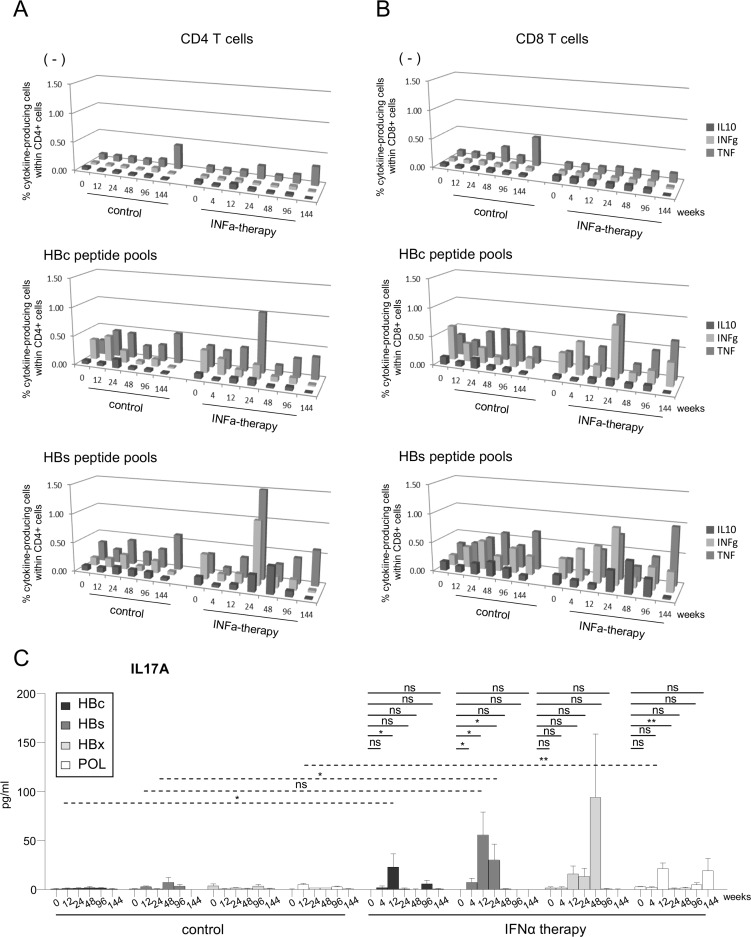
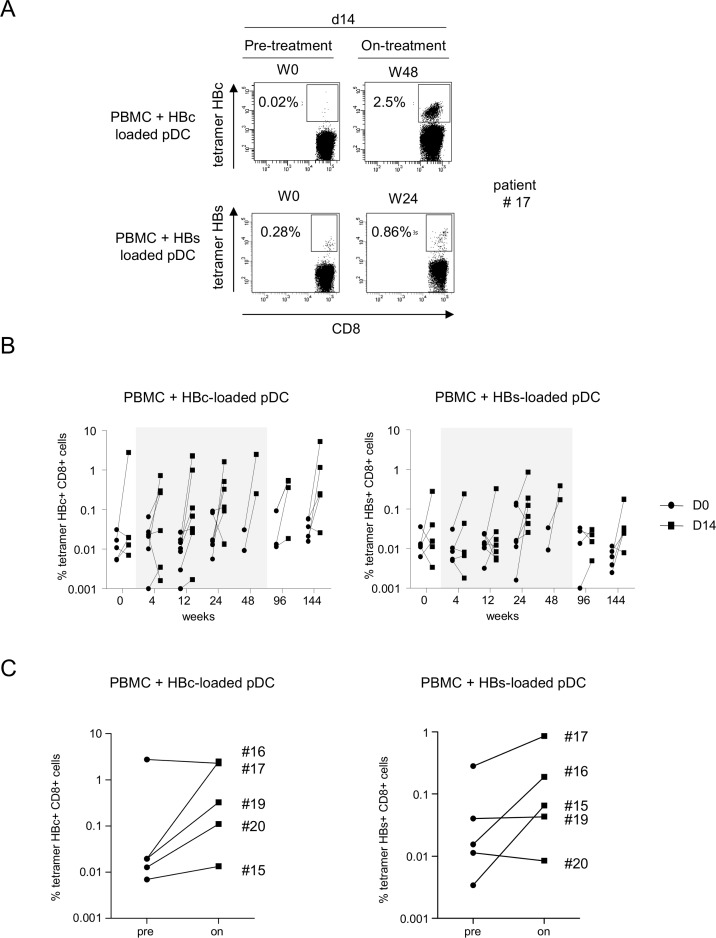
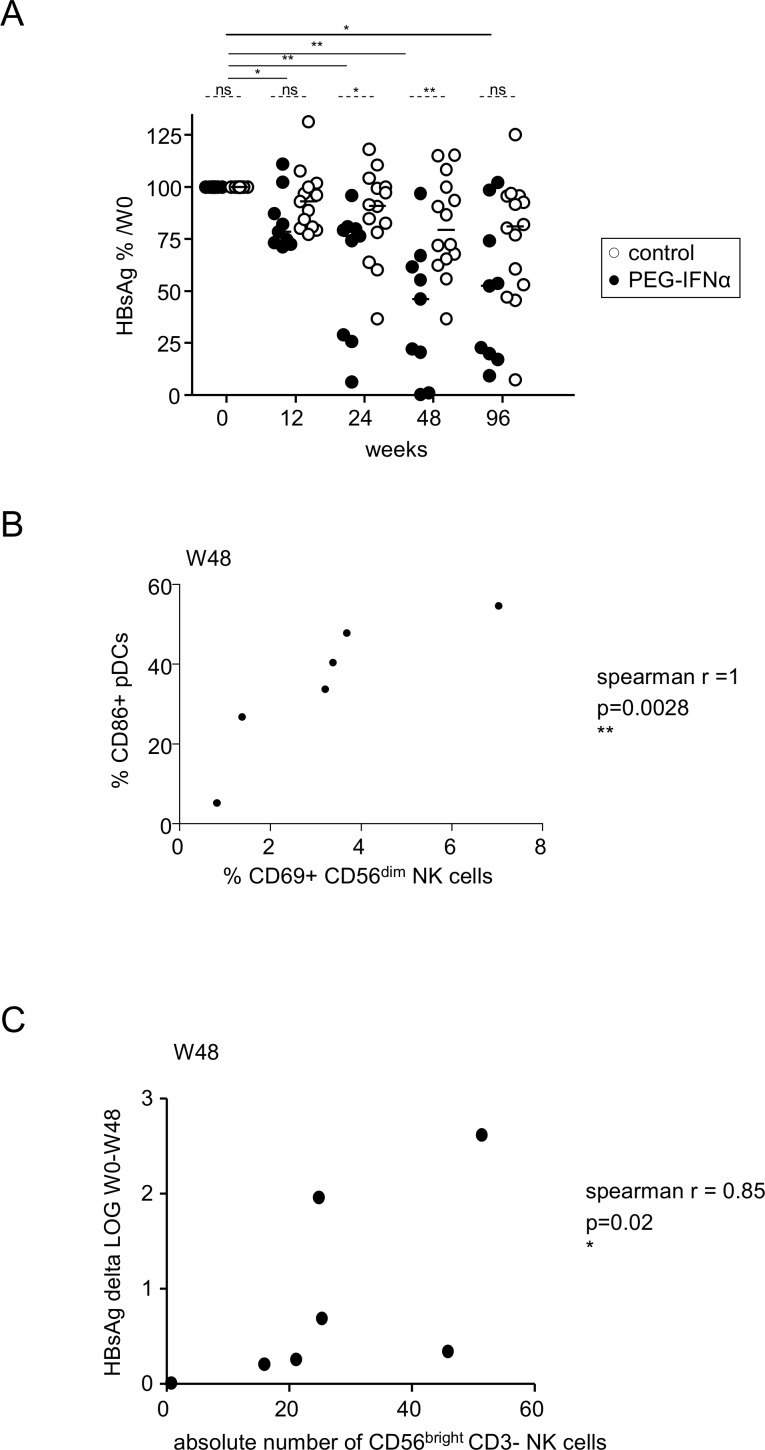
Pegylated interferon α-2a (Peg-IFN-α) represents a therapeutic alternative to the prolonged use of nucleos(t)ide analog (NA) in chronic hepatitis B (CHB) infection. The mechanisms leading to a positive clinical outcome remain unclear. As immune responses are critical for virus control, we investigated the effects of Peg-IFN-α on both innate and adaptive immunity, and related it to the clinical evolution. The phenotypic and functional features of the dendritic cells (DCs), natural killer (NK) cells and HBV-specific CD4/CD8 T cells were analyzed in HBeAg-negative CHB patients treated for 48-weeks with NA alone or together with Peg-IFN-α, before, during and up to 2-years after therapy. Peg-IFN-α induced an early activation of DCs, a potent expansion of the CD56bright NK subset, and enhanced the activation and functionality of the CD56dim NK subset. Peg-IFN-α triggered an increase in the frequencies of Th1- and Th17-oriented HBV-specific CD4/CD8 T cells. Peg-IFN-α reversed the unresponsiveness of patients to a specific stimulation. Most of the parameters returned to baseline after the stop of Peg-IFN-α therapy. Peg-IFN-α impacts both innate and adaptive immunity, overcoming dysfunctional immune responses in CHB patients. These modulations were not associated with seroconversion, which questioned the benefit of the add-on Peg-IFN-α treatment.
Conflict of interest statement
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
