

CTLA4 as Immunological Checkpoint in the Development of Multiple Sclerosis
- PMID: 27351142
- PMCID: PMC5129566
- DOI: 10.1002/ana.24715
CTLA4 as Immunological Checkpoint in the Development of Multiple Sclerosis
Abstract
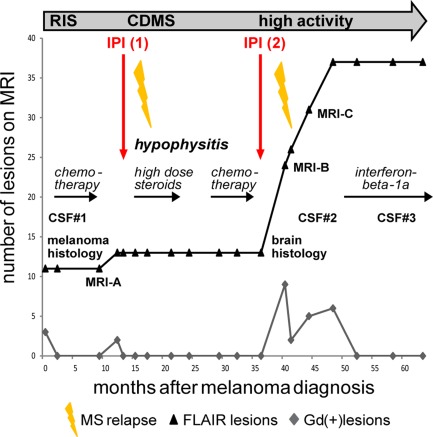
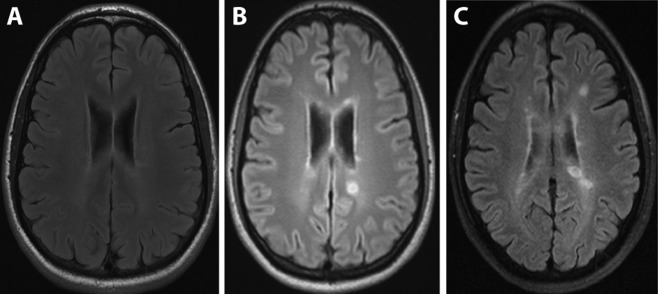
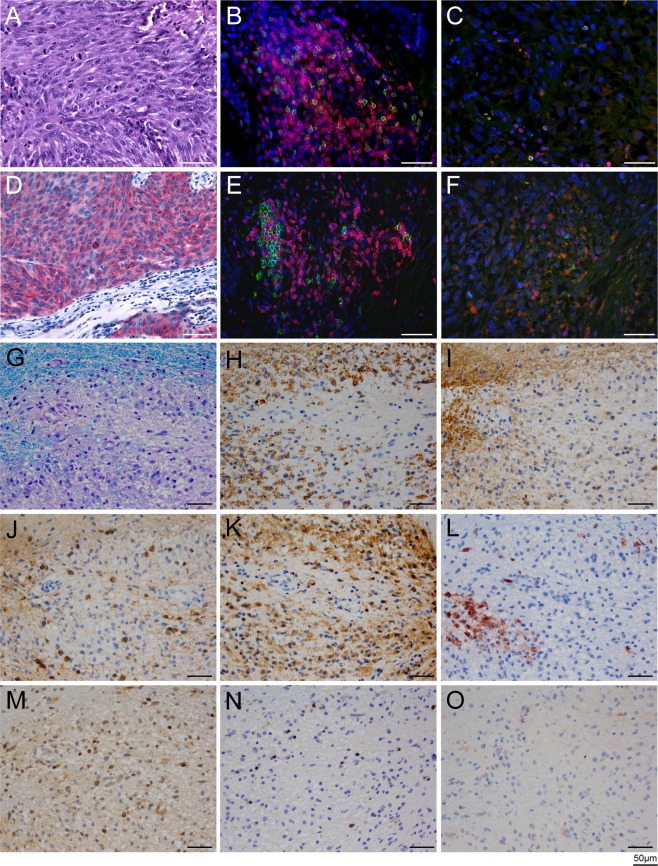
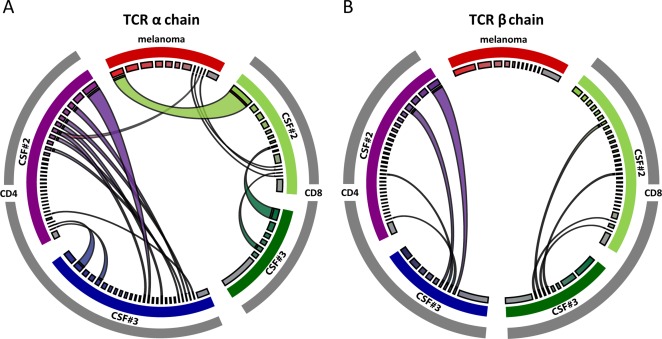
We investigated a patient who developed multiple sclerosis (MS) during treatment with the CTLA4-blocking antibody ipilimumab for metastatic melanoma. Initially he showed subclinical magnetic resonance imaging (MRI) changes (radiologically isolated syndrome). Two courses of ipilimumab were each followed by a clinical episode of MS, 1 of which was accompanied by a massive increase of MRI activity. Brain biopsy confirmed active, T-cell type MS. Quantitative next generation sequencing of T-cell receptor genes revealed distinct oligoclonal CD4(+) and CD8(+) T-cell repertoires in the primary melanoma and cerebrospinal fluid. Our results pinpoint the coinhibitory molecule CTLA4 as an immunological checkpoint and therapeutic target in MS. Ann Neurol 2016;80:294-300.
© 2016 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
