

Treatments for breast engorgement during lactation
- PMID: 27351423
- PMCID: PMC7388926
- DOI: 10.1002/14651858.CD006946.pub3
Treatments for breast engorgement during lactation
Update in
-
Treatments for breast engorgement during lactation.Cochrane Database Syst Rev. 2020 Sep 18;9(9):CD006946. doi: 10.1002/14651858.CD006946.pub4. Cochrane Database Syst Rev. 2020. PMID: 32944940 Free PMC article.
Abstract
Background: Breast engorgement is a painful condition affecting large numbers of women in the early postpartum period. It may lead to premature weaning, cracked nipples, mastitis and breast abscess. Various forms of treatment for engorgement have been studied but so far little evidence has been found on an effective intervention.
Objectives: This is an update of a systematic review first published by Snowden et al. in 2001 and subsequently published in 2010. The objective of this update is to seek new information on the best forms of treatment for breast engorgement in lactating women.
Search methods: We identified studies for inclusion through the Cochrane Pregnancy and Childbirth Group's Trials Register (30 June 2015) and searched reference lists of retrieved studies.
Selection criteria: Randomised and quasi-randomised controlled trials.
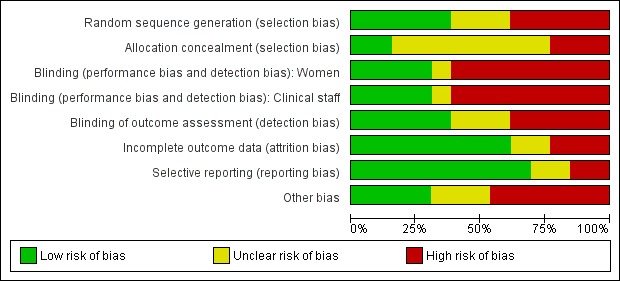
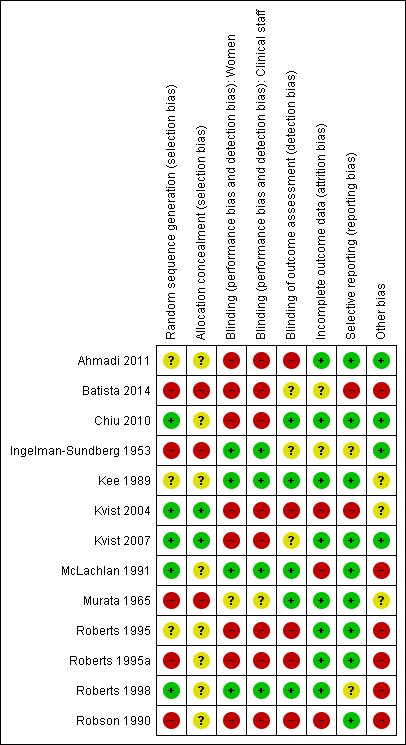
Data collection and analysis: Two review authors independently assessed trials for eligibility, extracted data and conducted 'Risk of bias' assessments. Where insufficient data were presented in trial reports, we attempted to contact study authors and obtain necessary information. We assessed the quality of the evidence using the GRADE approach.
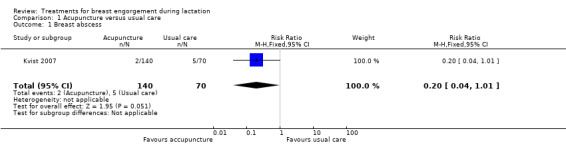
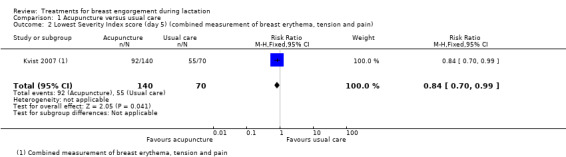
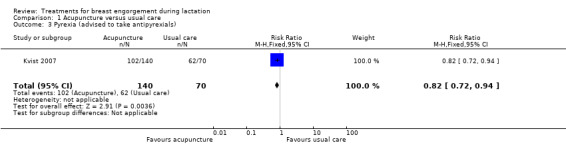
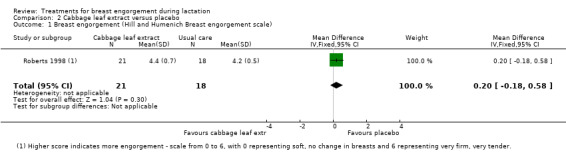
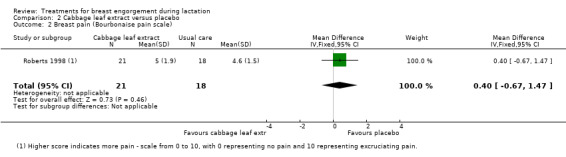
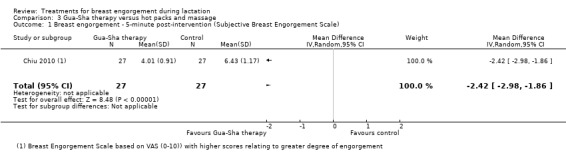
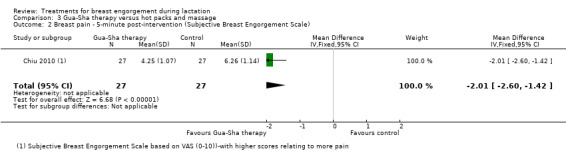
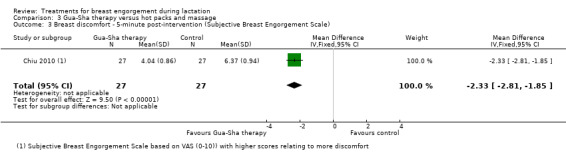
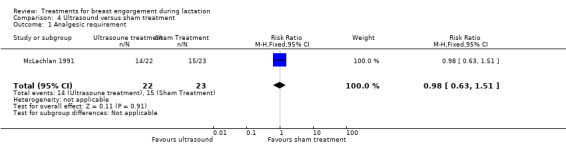
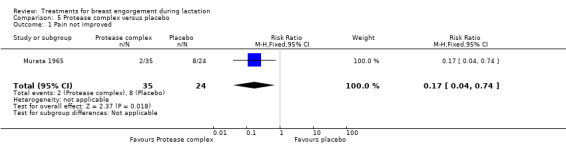
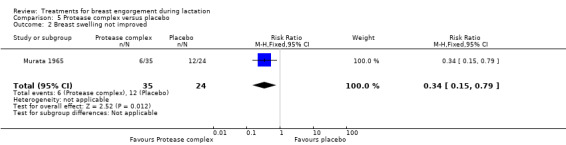
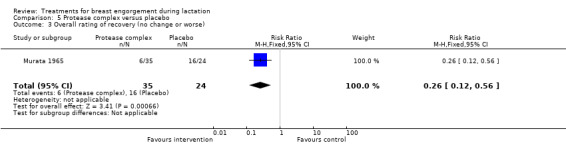
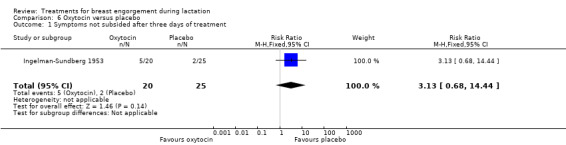
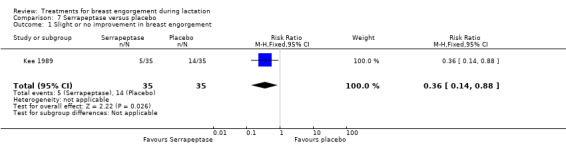
Main results: In total, we included 13 studies with 919 women. In 10 studies individual women were the unit of analysis and in three studies, individual breasts were the unit of analysis. Four out of 13 studies were funded by an agency with a commercial interest, two received charitable funding, and two were funded by government agencies.Trials examined interventions including non-medical treatments: cabbage leaves (three studies), acupuncture (two studies), ultrasound (one study), acupressure (one study), scraping therapy (Gua Sha) (one study), cold breast-packs and electromechanical massage (one study), and medical treatments: serrapeptase (one study), protease (one study) and subcutaneous oxytocin (one study). The studies were small and used different comparisons with only single studies contributing data to outcomes of this review. We were unable to pool results in meta-analysis and only seven studies provided outcome data that could be included in data and analysis. Non-medical No differences were observed in the one study comparing acupuncture with usual care (advice and oxytocin spray) (risk ratio (RR) 0.50, 95% confidence interval (CI) 0.13 to 1.92; one study; 140 women) in terms of cessation of breastfeeding. However, women in the acupuncture group were less likely to develop an abscess (RR 0.20, 95% CI 0.04 to 1.01; one study; 210 women), had less severe symptoms on day five (RR 0.84, 95% CI 0.70 to 0.99), and had a lower rate of pyrexia (RR 0.82, 95% CI 0.72 to 0.94) than women in the usual care group.In another study with 39 women comparing cabbage leaf extract with placebo, no differences were observed in breast pain (mean difference (MD) 0.40, 95% CI -0.67 to 1.47; low-quality evidence) or breast engorgement (MD 0.20, 95% CI -0.18 to 0.58; low-quality evidence). There was no difference between ultrasound and sham treatment in analgesic requirement (RR 0.98, 95% CI 0.63 to 1.51; one study; 45 women; low-quality evidence). A study comparing Gua-Sha therapy with hot packs and massage found a marked difference in breast engorgement (MD -2.42, 95% CI -2.98 to -1.86; one study; 54 women), breast pain (MD -2.01, 95% CI -2.60 to -1.42; one study; 54 women) and breast discomfort (MD -2.33, 95% CI -2.81 to -1.85; one study; 54 women) in favour of Gua-Sha therapy five minutes post-intervention, though both interventions significantly decreased breast temperature, engorgement, pain and discomfort at five and 30 minutes post-treatment.Results from individual trials that could not be included in data analysis suggested that there were no differences between room temperature and chilled cabbage leaves and between chilled cabbage leaves and gel packs, with all interventions producing some relief. Intermittent hot/cold packs applied for 20 minutes twice a day were found to be more effective than acupressure (P < 0.001). Acupuncture did not improve maternal satisfaction with breastfeeding. In another study, women who received breast-shaped cold packs were more likely to experience a reduction in pain intensity than women who received usual care; however, the differences between groups at baseline, and the failure to observe randomisation, make this study at high risk of bias. One study found a decrease in breast temperature (P = 0.03) following electromechanical massage and pumping in comparison to manual methods; however, the high level of attrition and alternating method of sequence generation place this study at high risk of bias. MedicalWomen treated with protease complex were less likely to have no improvement in pain (RR 0.17, 95% CI 0.04 to 0.74; one study; 59 women) and swelling (RR 0.34, 95% CI 0.15 to 0.79; one study; 59 women) on the fourth day of treatment and less likely to experience no overall change in their symptoms or worsening of symptoms (RR 0.26, 95% CI 0.12 to 0.56). It should be noted that it is more than 40 years since the study was carried out, and we are not aware that this preparation is used in current practice. Subcutaneous oxytocin provided no relief at all in symptoms at three days (RR 3.13, 95% CI 0.68 to 14.44; one study; 45 women).Serrapeptase was found to produce some relief in breast pain, induration and swelling, when compared to placebo, with a fewer number of women experiencing slight to no improvement in overallbreast engorgement, swelling and breast pain.Overall, the risk of bias of studies in the review is high. The overall quality as assessed using the GRADE approach was found to be low due to limitations in study design and the small number of women in the included studies, with only single studies providing data for analysis.
Authors' conclusions: Although some interventions such as hot/cold packs, Gua-Sha (scraping therapy), acupuncture, cabbage leaves and proteolytic enzymes may be promising for the treatment of breast engorgement during lactation, there is insufficient evidence from published trials on any intervention to justify widespread implementation. More robust research is urgently needed on the treatment of breast engorgement.
Conflict of interest statement
None known.
Figures


Update of
-
Treatments for breast engorgement during lactation.Cochrane Database Syst Rev. 2010 Sep 8;(9):CD006946. doi: 10.1002/14651858.CD006946.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2016 Jun 28;(6):CD006946. doi: 10.1002/14651858.CD006946.pub3. PMID: 20824853 Free PMC article. Updated.
References
References to studies included in this review
Ahmadi 2011 {published data only}
-
- Ahmadi M. The comparison of acupressure (jianjing point) and compress(hot and cold) on breast engorgement in lactating women. Iranian Clinical Trials Register (www.irct.ir/) (accessed 2 August 2012).
Batista 2014 {published data only}
-
- Batista dos Santos HA, Muniz de Moura MA, Souza MA, Nohama P. Evaluation of massage techniques and pumping in the treatment of breast engorgement by thermography [Evaluacion de las tecnicas de masaje y bombeo en el tratamiento de la congestion mamaria por termografia]. Revista Latino‐Americana de Enfermagem (RLAE) 2014;22(2):277‐85. - PMC - PubMed
Chiu 2010 {published data only}
-
- Chiu JY, Gau ML, Kuo SY, Chang YH, Kuo SC, Tu HC. Effects of Gua‐Sha therapy on breast engorgement: a randomized controlled trial. Journal of Nursing Research 2010;18(1):1‐10. - PubMed
Ingelman‐Sundberg 1953 {published data only}
-
- Ingelman‐Sundberg A. Early puerperal breast engorgement. Acta Paediatrica Scandinavica 1953;32:399‐402. - PubMed
Kee 1989 {published data only}
-
- Kee WH, Tan SL, Lee V, Samon YM. The treatment of breast engorgement with serrapeptase (Danzen): a randomized double‐blind controlled trial [The treatment of breast engorgement with serrapeptase (Danzen): a randomized double‐blind controlled trial]. Singapore Medical Journal 1989;30(1):48‐54. - PubMed
-
- Tan SL, Kee WH, Lee V, Salmon YM. The use of serratiopeptidase (Danzen) for the treatment of breast engorgement ‐ a randomised double‐blind controlled trial. Proceedings of the 24th British Congress of Obstetrics and Gynaecology;1986 April 15‐18; Cardiff, UK. 1986:246.
Kvist 2004 {published data only}
-
- Kvist LJ, Wilde Larsson B, Hall‐Lord ML, Rydhstroem H. Effects of acupuncture and care interventions on the outcome of inflammatory symptoms of the breast in lactating women. International Nursing Review 2004;51(1):56‐64. - PubMed
Kvist 2007 {published data only}
-
- Kvist LJ, Hall‐Lord ML, Rydhstroem H, Larsson BW. A randomised‐controlled trial in Sweden of acupuncture and care interventions for the relief of inflammatory symptoms of the breast during lactation. Midwifery 2007;23:184‐95. - PubMed
McLachlan 1991 {published data only}
-
- McLachlan Z, Milne EJ, Lumley J, Walker BL. Ultrasound treatment for breast engorgement: a randomised double blind trial. Australian Journal of Physiotherapy 1991;37(1):23‐9. - PubMed
-
- McLachlan Z, Milne EJ, Lumley J, Walker BL. Ultrasound treatment for breast engorgement: a randomised double blind trial. Breastfeeding Review 1993;2(7):316‐20. - PubMed
-
- McLachlan Z, Milne J, Lumley J. The efficacy of ultrasound as a treatment for severe breast engorgement. Tenth International Congress World Confederation for Physical Therapy; 1987 May 17‐22; Sydney, Australia. 1987:342‐6.
Murata 1965 {published data only}
-
- Murata T, Hanzawa M, Nomura Y. The clinical effects of "Protease complex" on postpartum breast engorgement (based on the double blind method). Journal of Japanese Obstetrical and Gynecological Society 1965;12(3):139‐47. - PubMed
Roberts 1995 {published data only}
-
- Roberts KL. A comparison of chilled cabbage leaves and chilled gelpaks in reducing breast engorgement. Journal of Human Lactation 1995;11(1):17‐20. - PubMed
Roberts 1995a {published data only}
-
- Roberts KL, Reiter M, Schuster D. A comparison of chilled and room temperature cabbage leaves in treating breast engorgement. Journal of Human Lactation 1995;11:191‐4. - PubMed
Roberts 1998 {published data only}
-
- Roberts KL, Reiter M, Schuster D. Effects of cabbage leaf extract on breast engorgement. Journal of Human Lactation 1998;14(3):231‐6. - PubMed
Robson 1990 {published data only}
-
- Robson BA. Breast Engorgement in Breastfeeding Mothers. [thesis]. Case Western Reserve University, 1990.
References to studies excluded from this review
Booker 1970 {published data only}
-
- Booker DE, Pahl IR, Forbes DA. Control of postpartum breast engorgement with oral contraceptives. II. American Journal of Obstetrics and Gynecology 1970;108:240‐2. - PubMed
Filteau 1999 {published data only}
Garry 1956 {published data only}
-
- Garry J. Estrogen‐androgen preparation for prevention of postpartum breast engorgement and lactation. Obstetrics & Gynecology 1956;7:422‐4. - PubMed
King 1958 {published data only}
-
- King AG. Prevention of puerperal breast engorgement with large doses of long‐acting estrogen. American Journal of Obstetrics and Gynecology 1958;78:80‐5. - PubMed
Nikodem 1993 {published data only}
-
- Danziger D, Gebka N, Nikodem C, Gulmezoglu M, Hofmeyr GJ. Do cabbage leaves prevent breast engorgement? Randomised, controlled study. Proceedings of the 12th Conference on Priorities in Perinatal Care; 1993; South Africa. 1993:114‐6.
-
- Nikodem VC, Danziger D, Gebka N, Gulmezoglu AM, Hofmeyr GJ. Do cabbage leaves prevent breast engorgement? a randomized, controlled study. Birth 1993;20(2):61‐4. - PubMed
Phillips 1975 {published data only}
-
- Phillips WP. Prevention of postpartum breast engorgement: double‐blind comparison of chlorotrianisene 72mg and placebo. Journal of the Arkansas Medical Society 1975;72:163‐7. - PubMed
Roser 1966 {published data only}
-
- Roser DM. Breast engorgement and postpartum fever. Obstetrics & Gynecology 1966;27:73‐7. - PubMed
Ryan 1962 {published data only}
-
- Ryan GM Jr, Brown DAJ. Intranasal syntocinon and postpartum breast engorgement. Obstetrics & Gynecology 1962;20:582‐4. - PubMed
Stenchever 1962 {published data only}
-
- Stenchever MA. Evaluation of chlorprophenpyridamine for prevention of postpartum breast engorgement. American Journal of Obstetrics and Gynecology 1962;840:969‐71. - PubMed
Additional references
ABM 2009
-
- The Academy of Breastfeeding Medicine Protocol Committee. ABM Clinical Protocol #20: Engorgement. Breastfeeding Medicine 2009;4(2):111‐3. - PubMed
Acarturk 2005
-
- Acarturk S, Gensel E, Tuncer I. An uncommon complication of secondary augmentation mammoplasty: bilaterally massive engorgement of breasts after pregnancy attributable to postinfection and blockage of mammary ducts. Aesthetic Plastic Surgery 2005;29(4):274‐9. - PubMed
Carletti 2011
-
- Carletti C, Pani P, Knowles A, Monasta L, Montico M, Cattaneo A. Breastfeeding to 24 months of age in the northeast of Italy: a cohort study. Breastfeeding Medicine 2011;6(4):177‐82. - PubMed
Core Curriculum 2013
-
- Mannel R, Martens PJ, Walker M. Core Curriculum for Lactation Consultant Practice. Third Edition. Burlington: Jones & Bartlett Learning, 2013.
Cotterman 2004
-
- Cotterman KJ. Reverse pressure softening: a simple tool to prepare areola for easier latching during engorgement. Journal of Human Lactation 2004;20(2):227‐37. - PubMed
Giugliani 2004
-
- Giugliani ER. Common problems during lactation and their management. Jornal de Pediatria 2004;80(5 Suppl):S147‐S154. - PubMed
Hale 2007
-
- Hale TW, Hartmann PE. Textbook of Human Lactation. First Edition. Amarillo: Hale Publishing, 2007.
Hauck 2011
-
- Hauck YL, Fenwick J, Dhaliwal SS, Butt J. A Western Australian survey of breastfeeding initiation, prevalence and early cessation patterns. Maternal Child Health Journal 2011;15(2):260‐8. - PubMed
Higgins 2011
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hill 1994
-
- Hill PD, Humenick SS. The occurrence of breast engorgement. Journal of Human Lactation 1994;10(2):79‐86. - PubMed
Humenick 1994
-
- Humenick SS, Hill PD, Anderson MA. Breast engorgement: patterns and selected outcomes. Journal of Human Lactation 1994;10(2):87‐93. - PubMed
Hure 2013
Liu 2013
-
- Liu P, Qiao L, Xu F, Zhang M, Wang Y, Binns C. Factors associated with breastfeeding duration: a 30‐month cohort study in northwest China. Journal of Human Lactation 2013;29(2):253‐9. - PubMed
Mass 2004
-
- Mass M. Breast pain: engorgement, nipple pain and mastitis. Clinical Obstetrics and Gynecology 2004;47(3):676‐82. - PubMed
NICE 2006
-
- Demott K, Bick D, Norman R, Ritchie G, Turnbull N, Adams C, et al. Clinical Guidelines and Evidence Review for Postnatal Care: Routine Postnatal Care of Recently Delivered Women and Their Babies. London: National Collaborating Centre For Primary Care And Royal College Of General Practitioners, 2006.
Odom 2013
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
WHO 2003
-
- World Health Organization. Global Strategy for Infant and Young Child Feeding. Geneva: WHO, 2003.
References to other published versions of this review
Mangesi 2010
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical