

Cadaveric aorta implantation for aortic graft infection
- PMID: 27351624
- PMCID: PMC4925903
- DOI: 10.1016/j.ijscr.2016.06.012
Cadaveric aorta implantation for aortic graft infection
Abstract
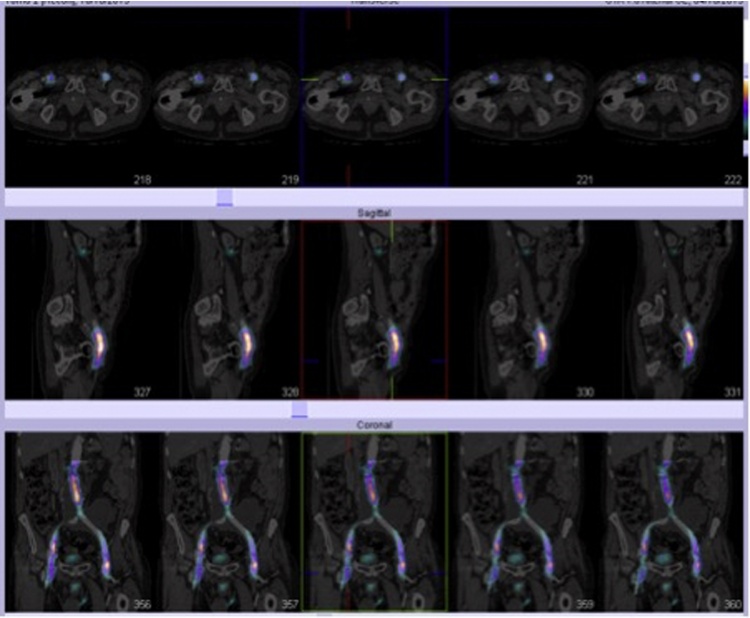
This case report describes a 73-year-old gentleman who underwent explantation of an infected prosthetic aorto-iliac graft and replacement with a cryopreserved thoracic and aorto-iliac allograft. The patient has been followed up a for more than a year after surgery and remains well. After elective tube graft repair of his abdominal aortic aneurysm (AAA) in 2003, he presented to our unit in 2012 in cardiac arrest as a result of a rupture of the distal graft suture line due to infection. After resuscitation he underwent aorto-bifemoral grafting using a cuff of the original aortic graft proximally. Distally the new graft was anastomosed to his common femoral arteries, with gentamicin beads left in situ. Post discharge the patient was kept under close surveillance with serial investigations including nuclear scanning, however it became apparent that his new graft was infected and that he would require aortic graft replacement, an operation with a mortality of at least 50%. The patient underwent the operation and findings confirmed a synthetic graft infection. This tube graft was explanted and a cryopreserved aorta was used to the refashion the abdominal aorta and its bifurcation. The operation required a return to theatre day one post operatively for a bleeding side branch, which was repaired. The patient went on to make a full recovery stepping down from the intensive therapy unit day 6 post operatively and went on to be discharged 32 days after his cryopreserved aorta implantation.
Keywords: Aortic graft; Cadaveric aorta; Infection; Transplant; Vascular surgery.
Copyright © 2016 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures







Similar articles
-
[Surgery of abdominal aorta with horseshoe kidney].Srp Arh Celok Lek. 1997 Jan-Feb;125(1-2):36-44. Srp Arh Celok Lek. 1997. PMID: 17974353 Serbian.
-
[Prosthetic repair of the aorta with a cadaveric homograft for infection of bifurcated synthetic vascular prosthesis].Angiol Sosud Khir. 2021;27(3):132-139. doi: 10.33529/ANGIO2021315. Angiol Sosud Khir. 2021. PMID: 34528597 Russian.
-
[Aorto-enteric fistulas].Srp Arh Celok Lek. 2001 Jul-Aug;129(7-8):183-93. Srp Arh Celok Lek. 2001. PMID: 11797448 Serbian.
-
Aorto-enteric fistula after endovascular abdominal aortic aneurysm repair: case report and review.Eur J Vasc Endovasc Surg. 2009 Apr;37(4):401-6. doi: 10.1016/j.ejvs.2008.11.037. Epub 2009 Feb 10. Eur J Vasc Endovasc Surg. 2009. PMID: 19211278 Review.
-
Complex abdominal and thoracoabdominal aortic aneurysm reconstruction.Surg Today. 1995;25(2):99-106. doi: 10.1007/BF00311078. Surg Today. 1995. PMID: 7772928 Review.
Cited by
-
Clinical outcomes of in situ graft reconstruction in treating infected abdominal aortic stent grafts following endovascular aortic aneurysm repair: a single-center experience.Ann Surg Treat Res. 2023 Jun;104(6):339-347. doi: 10.4174/astr.2023.104.6.339. Epub 2023 Jun 7. Ann Surg Treat Res. 2023. PMID: 37337602 Free PMC article.
References
-
- O’Connor S., Andrew P., Batt M., Becquemin J.P. A systematic review and meta-analysis of treatments for aortic graft infection. J. Vasc. Surg. 2006;44:38–45. - PubMed
-
- Hallett J.W., Marshall D.M., Petterson T.M., Gray D.T., Bower T.C., Cherry K.J., Jr. Graft-related complications after abdominal aortic aneurysm repair: reassurance from a 36-year population-based experience. J. Vasc. Surg. 1997;25:277–286. - PubMed
-
- Johnson K.W. Multicenter prospective study of nonruptured abdominal aortic aneurysms: II. Variables predicting morbidity and mortality. J. Vasc. Surg. 1989;9:427. - PubMed
-
- McCready R.A., Bryant M.A., Divelbiss J.L., Chess B.A., Chitwood R.W., Paget D.S. Arterial infections in the new millennium: an old problem revisited. Ann. Vasc. Surg. 2006;20:590–595. - PubMed
-
- O’Hara P.J., Hertzer N.R., Beven E.G., Krajewski L.P. Surgical management of infected abdominal aortic grafts: review of a 25-year experience. J. Vasc. Surg. 1986;3:725–731. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
