

Estimating the prevalence of hematological malignancies and precursor conditions using data from Haematological Malignancy Research Network (HMRN)
- PMID: 27351920
- PMCID: PMC4958130
- DOI: 10.1007/s10552-016-0780-z
Estimating the prevalence of hematological malignancies and precursor conditions using data from Haematological Malignancy Research Network (HMRN)
Abstract
Objective: Well-established cancer registries that routinely link to death registrations can estimate prevalence directly by counting patients alive at a particular point in time (observed prevalence). Such direct methods can only provide prevalence for the years over which the registry has been operational. Time-defined estimates, including 5- and 10-year prevalence, may however underestimate the total cancer burden, and compared with other cancers, there is a lack of accurate information on the total prevalence of hematological malignancy subtypes. Accordingly, we aimed to estimate prevalence (observed and total prevalence) of hematological malignancies and precursor conditions by clinically meaningful subtypes using data from the UK's specialist population-based register, the Haematological Malignancy Research Network ( www.hmrn.org ).
Methods: Observed and total prevalences were estimated from 15,810 new diagnoses of hematological malignancies from 2004 to 2011 and followed up to the 31 August 2011 (index data). Observed prevalence was calculated by the counting method, and a method based on modelling incidence and survival was used to estimate total prevalence. Estimates were made according to current disease classification for the HMRN region and for the UK.
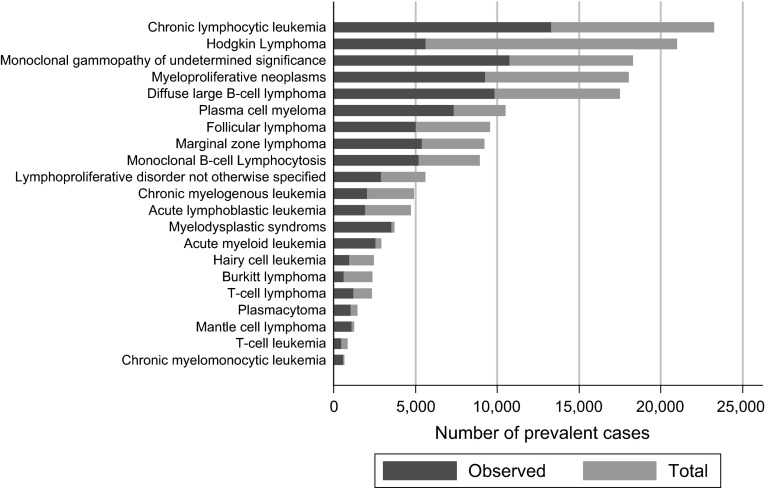
Results: The overall observed and total prevalence rates were 281.9 and 548.8 per 100,000, respectively; the total number of observed and total prevalent cases in the UK was estimated as 165,841 and 327,818 cases, as expected variation existed by disease subtype reflecting the heterogeneity in underlying disease incidence, survival and age distribution of hematological cancers.
Conclusions: This study demonstrates the importance of estimating 'total' prevalence rather than 'observed' prevalence by current disease classification (ICD-O-3), particularly for subtypes that have a more indolent nature and for those that are curable. Importantly, these analyses demonstrate that relying on observed prevalence alone would result in a significant underestimation of the relative burden of some subtypes. While many of these cases may be considered cured and no longer being actively treated, people in this survivorship phase may have long-term medical needs and accordingly, it is important to provide accurate counts to allow for healthcare planning.
Keywords: Cancer registry; Epidemiology; Leukemia; Lymphoma; Myeloma; Prevalence.
Figures


References
-
- Silva I. Cancer epidemiology: principles and methods, 2nd revised. Lyon: World Health Organization; 1999.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
