

Association between intensive care unit transfer delay and hospital mortality: A multicenter investigation
- PMID: 27352032
- PMCID: PMC5119525
- DOI: 10.1002/jhm.2630
Association between intensive care unit transfer delay and hospital mortality: A multicenter investigation
Abstract
Background: Previous research investigating the impact of delayed intensive care unit (ICU) transfer on outcomes has utilized subjective criteria for defining critical illness.
Objective: To investigate the impact of delayed ICU transfer using the electronic Cardiac Arrest Risk Triage (eCART) score, a previously published early warning score, as an objective marker of critical illness.
Design: Observational cohort study.
Setting: Medical-surgical wards at 5 hospitals between November 2008 and January 2013.
Patients: Ward patients.
Intervention: None.
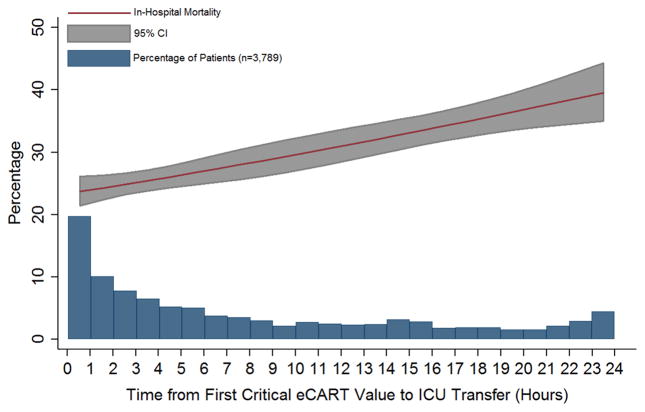
Measurements: eCART scores were calculated for all patients. The threshold with a specificity of 95% for ICU transfer (eCART ≥ 60) denoted critical illness. A logistic regression model adjusting for age, sex, and surgical status was used to calculate the association between time to ICU transfer from first critical eCART value and in-hospital mortality.
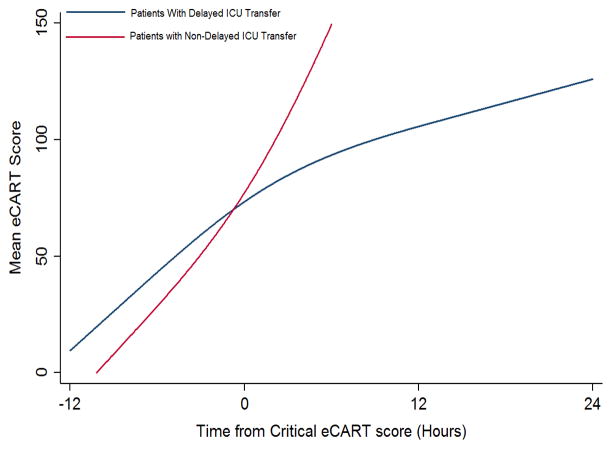
Results: A total of 3789 patients met the critical eCART threshold before ICU transfer, and the median time to ICU transfer was 5.4 hours. Delayed transfer (>6 hours) occurred in 46% of patients (n = 1734) and was associated with increased mortality compared to patients transferred early (33.2% vs 24.5%, P < 0.001). Each 1-hour increase in delay was associated with an adjusted 3% increase in odds of mortality (P < 0.001). In patients who survived to discharge, delayed transfer was associated with longer hospital length of stay (median 13 vs 11 days, P < 0.001).
Conclusions: Delayed ICU transfer is associated with increased hospital length of stay and mortality. Use of an evidence-based early warning score, such as eCART, could lead to timely ICU transfer and reduced preventable death. Journal of Hospital Medicine 2016;11:757-762. © 2016 Society of Hospital Medicine.
© 2016 Society of Hospital Medicine.
Conflict of interest statement
and Source of Funding: This research was funded in part by an institutional Clinical and Translational Science Award grant (UL1 RR024999; PI: Dr. Julian Solway). Dr. Churpek is supported by a career development award from the National Heart, Lung, and Blood Institute (K08 HL121080). Drs. Churpek and Edelson have a patent pending (ARCD. P0535US.P2) for risk stratification algorithms for hospitalized patients. In addition, Dr. Edelson has received research support from Philips Healthcare (Andover, MA), research support from the American Heart Association (Dallas, TX) and Laerdal Medical (Stavanger, Norway). She has ownership interest in Quant HC (Chicago, IL), which is developing products for risk stratification of hospitalized patients.
Figures
References
-
- Simchen E, Sprung CL, Galai N, et al. Survival of critically ill patients hospitalized in and out of intensive care units under paucity of intensive care unit beds. Critical care medicine. 2004 Aug;32(8):1654–1661. - PubMed
-
- Robert R, Reignier J, Tournoux-Facon C, et al. Refusal of intensive care unit admission due to a full unit: impact on mortality. American journal of respiratory and critical care medicine. 2012 May 15;185(10):1081–1087. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
