

In Vitro Assessment of Combinations of Enterovirus Inhibitors against Enterovirus 71
- PMID: 27353263
- PMCID: PMC4997834
- DOI: 10.1128/AAC.01073-16
In Vitro Assessment of Combinations of Enterovirus Inhibitors against Enterovirus 71
Abstract
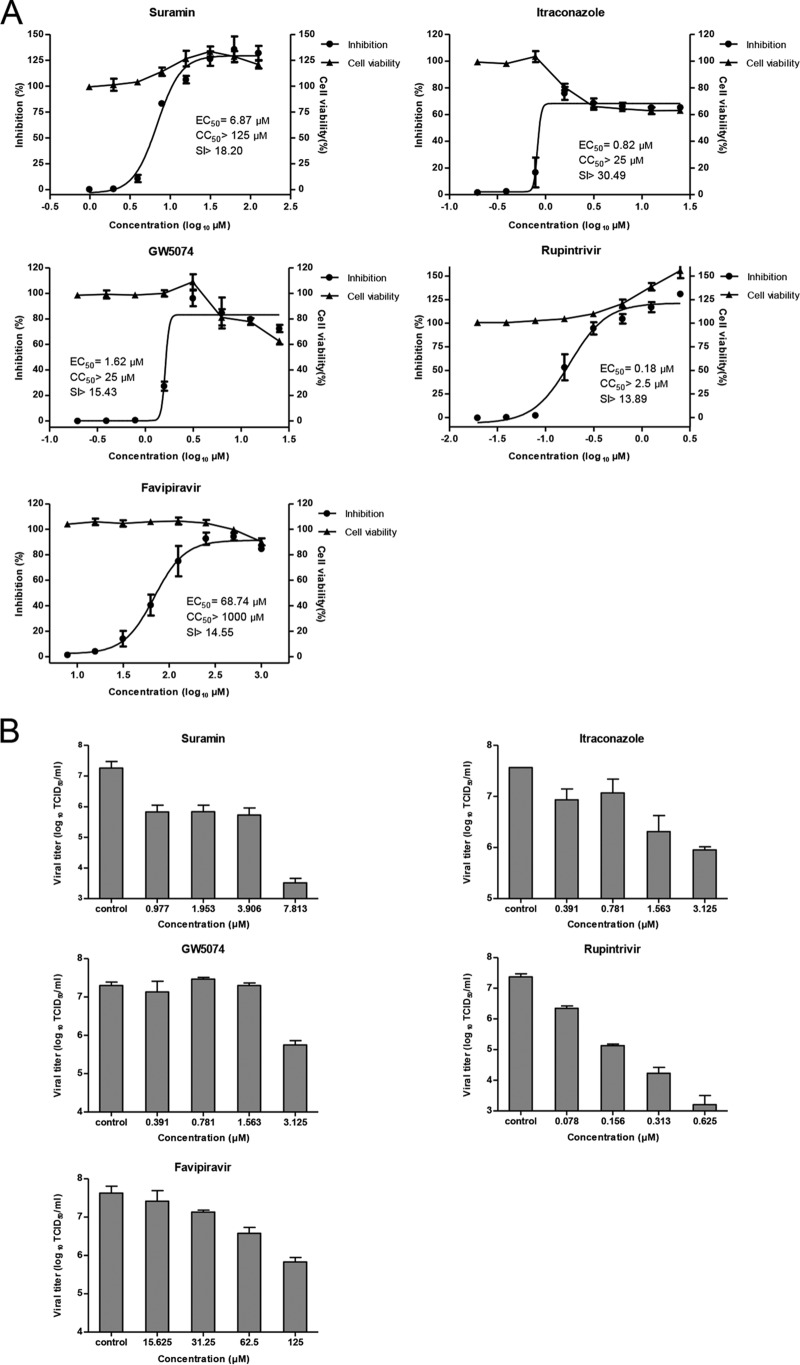
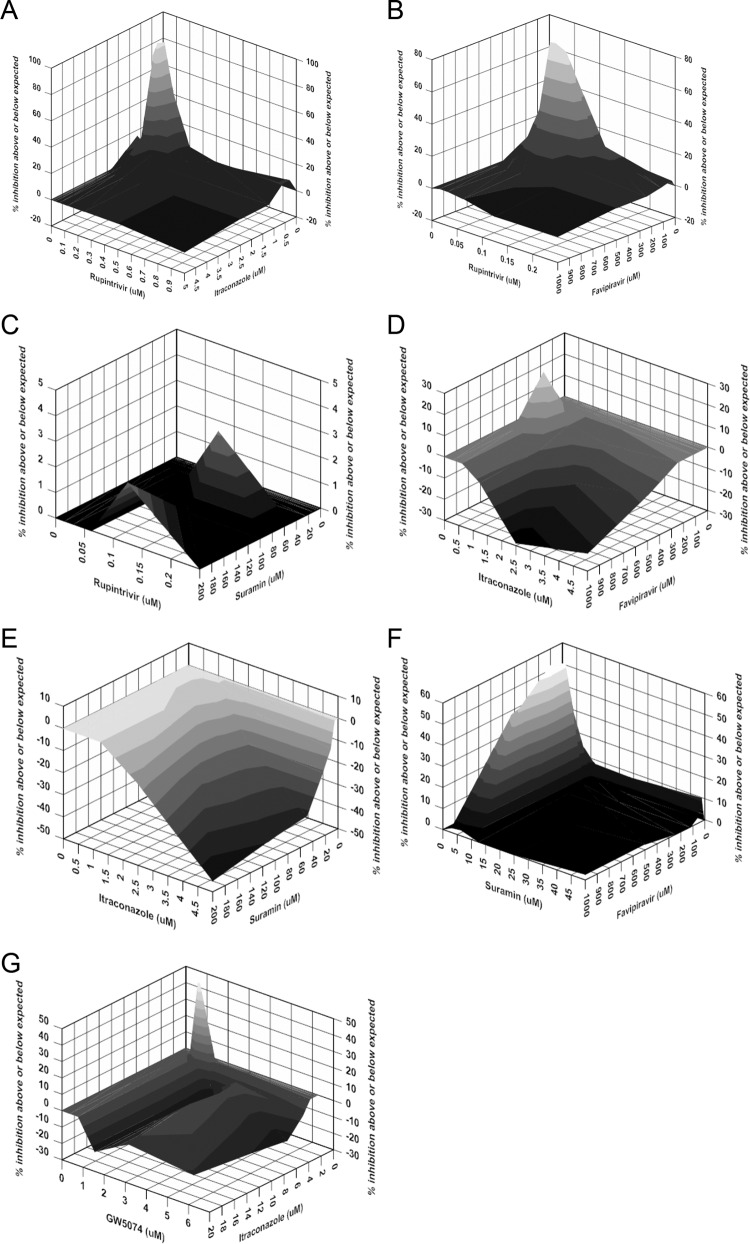
Enterovirus 71 (EV-A71) is a major causative pathogen of hand, foot, and mouth disease (HFMD) epidemics. No antiviral therapies are currently available for treating EV-A71 infections. Here, we selected five reported enterovirus inhibitors (suramin, itraconazole [ITZ], GW5074, rupintrivir, and favipiravir) with different mechanisms of action to test their abilities to inhibit EV-A71 replication alone and in combination. All selected compounds have anti-EV-A71 activities in cell culture. The combination of rupintrivir and ITZ or favipiravir was synergistic, while the combination of rupintrivir and suramin was additive. The combination of suramin and favipiravir exerted a strong synergistic antiviral effect. The observed synergy was not due to cytotoxicity, as there was no significant increase in cytotoxicity when compounds were used in combinations at the tested doses. To investigate the potential inhibitory mechanism of favipiravir against enterovirus, two favipiravir-resistant EV-A71 variants were independently selected, and both of them carried an S121N mutation in the finger subdomain of the 3D polymerase. Reverse engineering of this 3D S121N mutation into an infectious clone of EV-A71 confirmed the resistant phenotype. Moreover, viruses resistant to ITZ or favipiravir remained susceptible to other inhibitors. Most notably, combined with ITZ, rupintrivir prevented the development of ITZ-resistant variants. Taken together, these results provide a rational basis for the design of combination regimens for use in the treatment of EV-A71 infections.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures


References
-
- Zhang Q, Macdonald NE, Smith JC, Cai K, Yu H, Li H, Lei C. 2014. Severe enterovirus type 71 nervous system infections in children in the Shanghai region of China: clinical manifestations and implications for prevention and care. Pediatr Infect Dis J 33:482–487. doi:10.1097/INF.0000000000000194. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
