

Can SLE classification rules be effectively applied to diagnose unclear SLE cases?
- PMID: 27353506
- PMCID: PMC5192007
- DOI: 10.1177/0961203316655212
Can SLE classification rules be effectively applied to diagnose unclear SLE cases?
Abstract
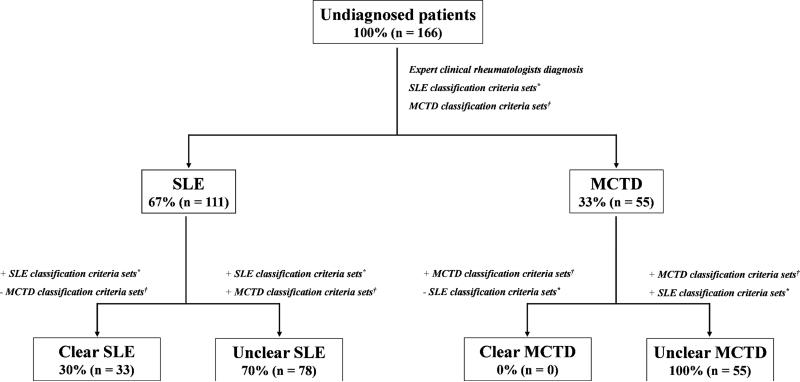
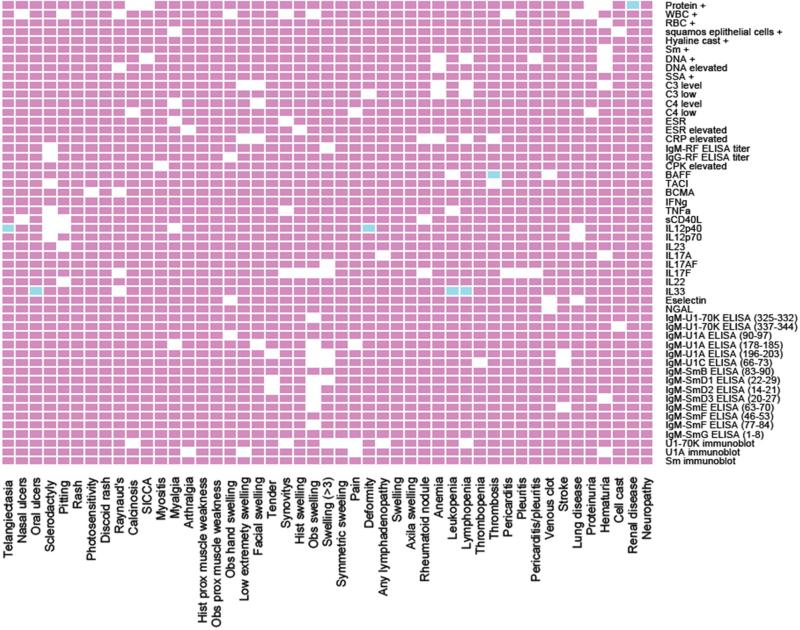
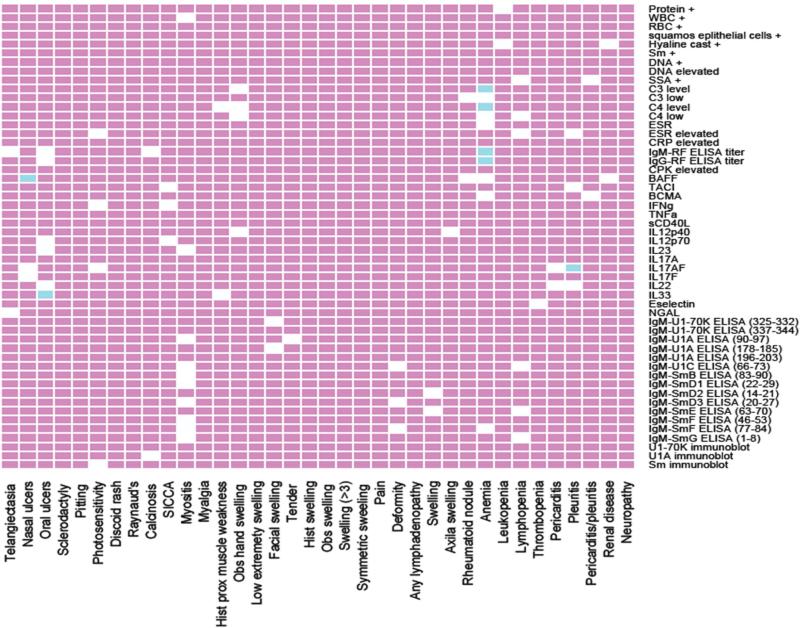
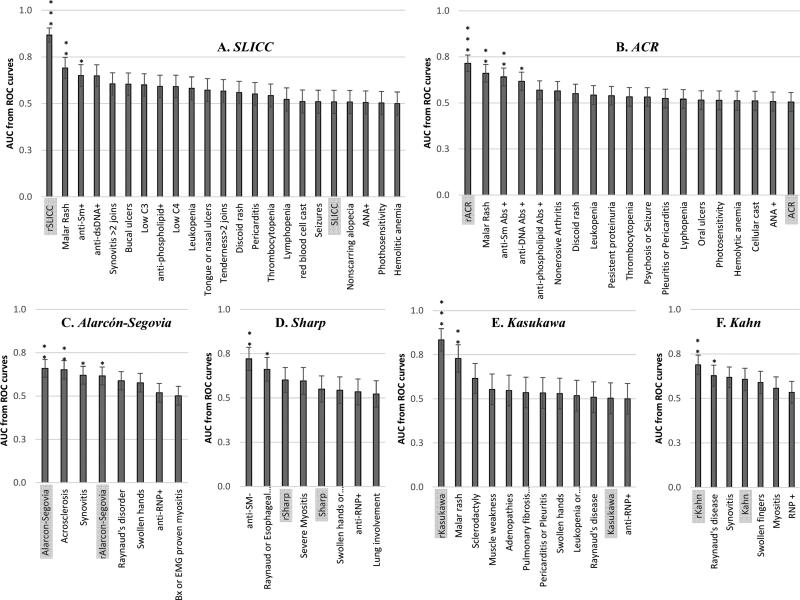
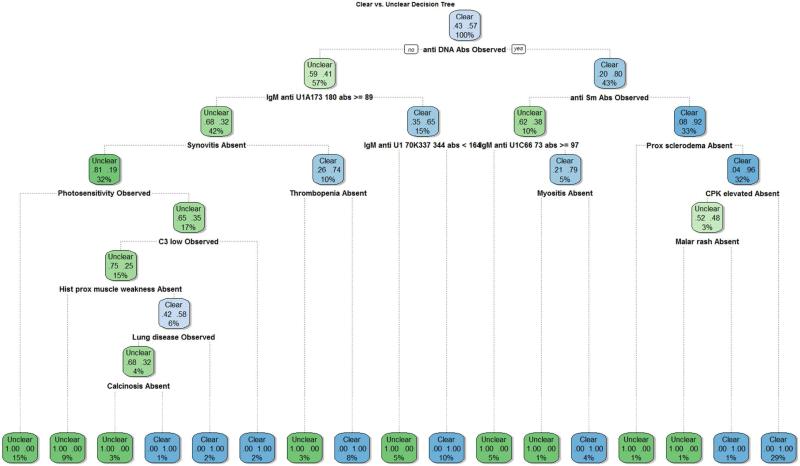
Objective The objective of this paper is to develop novel classification criteria to distinguish between unclear systemic lupus erythematosus (SLE) and mixed connective tissue disease (MCTD) cases. Methods A total of 205 variables from 111 SLE and 55 MCTD patients were evaluated to uncover unique molecular and clinical markers for each disease. Binomial logistic regressions (BLRs) were performed on currently used SLE and MCTD classification criteria sets to obtain six reduced models with power to discriminate between unclear SLE and MCTD patients that were confirmed by receiving operating characteristic (ROC) curve. Decision trees were employed to delineate novel classification rules to discriminate between unclear SLE and MCTD patients. Results SLE and MCTD patients exhibited contrasting molecular markers and clinical manifestations. Furthermore, reduced models highlighted SLE patients exhibiting prevalence of skin rashes and renal disease while MCTD cases show dominance of myositis and muscle weakness. Additionally decision tree analyses revealed a novel classification rule tailored to differentiate unclear SLE and MCTD patients (Lu-vs-M) with an overall accuracy of 88%. Conclusions Validation of our novel proposed classification rule (Lu-vs-M) includes novel contrasting characteristics (calcinosis, CPK elevated and anti-IgM reactivity for U1-70K, U1A and U1C) between SLE and MCTD patients and showed a 33% improvement in distinguishing these disorders when compared to currently used classification criteria sets. Pending additional validation, our novel classification rule is a promising method to distinguish between patients with unclear SLE and MCTD diagnosis.
Keywords: Mixed connective tissue disease (MCTD); autoimmune disorders; classification criteria; diagnosis; systemic lupus erythematosus (SLE).
Figures

Similar articles
-
The impact of anti-U1-RNP positivity: systemic lupus erythematosus versus mixed connective tissue disease.Rheumatol Int. 2018 Jul;38(7):1169-1178. doi: 10.1007/s00296-018-4059-4. Epub 2018 May 23. Rheumatol Int. 2018. PMID: 29796907 Review.
-
Differential immunoglobulin class-mediated responses to components of the U1 small nuclear ribonucleoprotein particle in systemic lupus erythematosus and mixed connective tissue disease.Lupus. 2013 Nov;22(13):1371-81. doi: 10.1177/0961203313508444. Lupus. 2013. PMID: 24158973 Free PMC article.
-
An external validation study of a classification of mixed connective tissue disease and systemic lupus erythematosus patients.J Appl Meas. 2012;13(2):205-16. J Appl Meas. 2012. PMID: 22805362
-
Diagnosis and risk stratification in patients with anti-RNP autoimmunity.Lupus. 2015 Sep;24(10):1057-66. doi: 10.1177/0961203315575586. Epub 2015 Mar 2. Lupus. 2015. PMID: 25736140 Free PMC article.
-
The diagnosis and classification of mixed connective tissue disease.J Autoimmun. 2014 Feb-Mar;48-49:46-9. doi: 10.1016/j.jaut.2014.01.008. Epub 2014 Jan 22. J Autoimmun. 2014. PMID: 24461387 Review.
Cited by
-
Low Expression and Clinical Value of hsa_circ_0049224 and has_circ_0049220 in Systemic Lupus Erythematous Patients.Med Sci Monit. 2018 Apr 2;24:1930-1935. doi: 10.12659/msm.906507. Med Sci Monit. 2018. PMID: 29606700 Free PMC article.
-
Validation of the new classification criteria for systemic lupus erythematosus on a patient cohort from a national referral center: a retrospective study.Croat Med J. 2019 Aug 31;60(4):333-344. doi: 10.3325/CroatMedJ_60_0325. Croat Med J. 2019. PMID: 31483119 Free PMC article.
-
Unraveling Complexity: A Case of Possible Overlapping Between Mixed Connective Tissue Disease and Systemic Lupus Erythematosus With Renal Involvement.Cureus. 2024 May 22;16(5):e60839. doi: 10.7759/cureus.60839. eCollection 2024 May. Cureus. 2024. PMID: 38910663 Free PMC article.
-
The impact of anti-U1-RNP positivity: systemic lupus erythematosus versus mixed connective tissue disease.Rheumatol Int. 2018 Jul;38(7):1169-1178. doi: 10.1007/s00296-018-4059-4. Epub 2018 May 23. Rheumatol Int. 2018. PMID: 29796907 Review.
References
-
- Sharp GC, Irvin WS, Tan EM, Gould RG, Holman HR. Mixed connective tissue diseaseAan apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972;52:148–159. - PubMed
-
- Steiner G, Skriner K, Hassfeld W, Smolen JS. Clinical and immunological aspects of autoantibodies to RA33/hnRNP-A/B proteins--a link between RA, SLE and MCTD. Mol Biol Rep. 1996;23:167–171. - PubMed
-
- Luyckx A, Westhovens R, Oris E, Papisch W, Bossuyt X. Clinical relevance of measurement of antibodies to individual snU1-RNP proteins. Clin Chem. 2015;51:1888–1890. - PubMed
-
- Vlachoyiannopoulos PG, Guialis A, Tzioufas G, Moutsopoulos HM. Predominance of IgM anti-U1RNP antibodies in patients with systemic lupus erythematosus. Br J Rheumatol. 1996;35:534–541. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
