

Abnormal right ventricular-pulmonary artery coupling with exercise in heart failure with preserved ejection fraction
- PMID: 27354047
- PMCID: PMC8483148
- DOI: 10.1093/eurheartj/ehw241
Abnormal right ventricular-pulmonary artery coupling with exercise in heart failure with preserved ejection fraction
Abstract
Background: Exercise intolerance is common in people with heart failure and preserved ejection fraction (HFpEF). Right ventricular (RV) dysfunction has been shown at rest in HFpEF but little data are available regarding dynamic RV-pulmonary artery (PA) coupling during exercise.
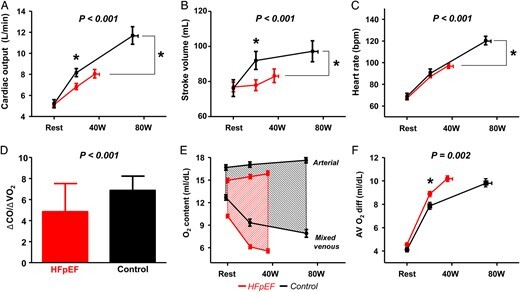
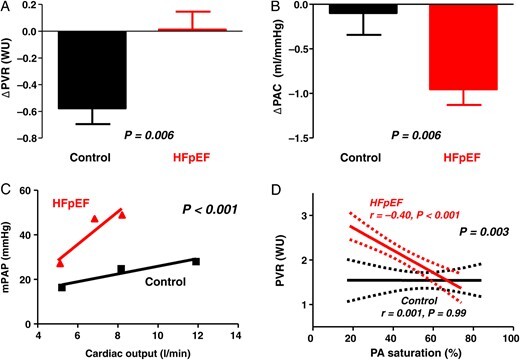
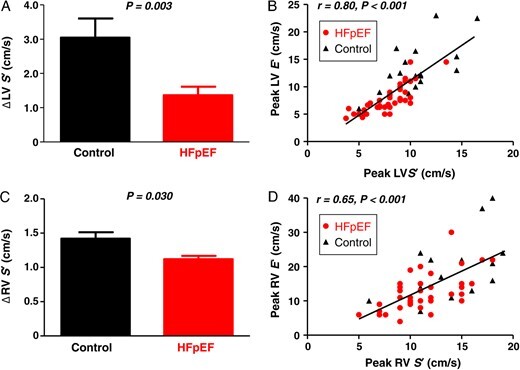
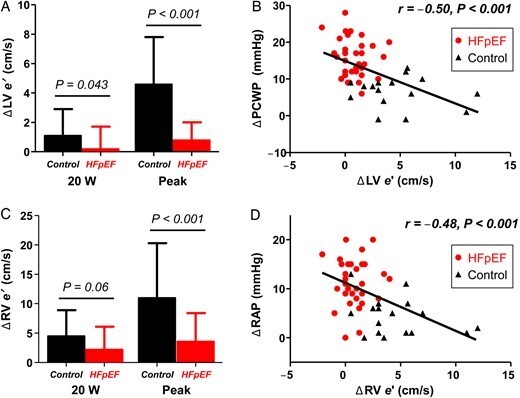
Methods and results: Subjects with HFpEF (n = 50) and controls (n = 24) prospectively underwent invasive cardiopulmonary exercise testing using high-fidelity micromanometer catheters along with simultaneous assessment of RV and left ventricular (LV) mechanics by echocardiography. Compared with controls at rest, subjects with HFpEF displayed preserved RV systolic and diastolic mechanics (RV s' and e'), impaired LV s' and e', higher biventricular filling pressures, and higher pulmonary artery pressures. On exercise, subjects with HFpEF displayed less increase in stroke volume, heart rate, and cardiac output (CO), with blunted increase in CO relative to O2 consumption (VO2). Enhancement in RV systolic and diastolic function on exercise was impaired in HFpEF compared with controls. Exercise-induced PA vasodilation was reduced in HFpEF in correlation with greater venous hypoxia. Elevations in biventricular filling pressures and limitations in CO reserve were strongly correlated with abnormal enhancement in ventricular mechanics in the RV and LV during stress.
Conclusions: In addition to limited LV reserve, patients with HFpEF display impaired RV reserve during exercise that is associated with high filling pressures and inadequate CO responses. These findings highlight the importance of biventricular dysfunction in HFpEF and suggest that novel therapies targeting myocardial reserve in both the left and right heart may be effective to improve clinical status.
Keywords: Diastolic function; Exercise; Haemodynamics; Heart failure; Heart failure with preserved ejection fraction; Pulmonary hypertension; Right ventricular function.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006;355:251–259. - PubMed
-
- Maeder MT, Thompson BR, Brunner-La Rocca HP, Kaye DM. Hemodynamic basis of exercise limitation in patients with heart failure and normal ejection fraction. J Am Coll Cardiol 2010;56:855–863. - PubMed
-
- Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, Kass DA. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation 2006;114:2138–2147. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
