

An Expression Signature as an Aid to the Histologic Classification of Non-Small Cell Lung Cancer
- PMID: 27354471
- PMCID: PMC5492382
- DOI: 10.1158/1078-0432.CCR-15-2900
An Expression Signature as an Aid to the Histologic Classification of Non-Small Cell Lung Cancer
Abstract
Purpose: Most non-small cell lung cancers (NSCLC) are now diagnosed from small specimens, and classification using standard pathology methods can be difficult. This is of clinical relevance as many therapy regimens and clinical trials are histology dependent. The purpose of this study was to develop an mRNA expression signature as an adjunct test for routine histopathologic classification of NSCLCs.
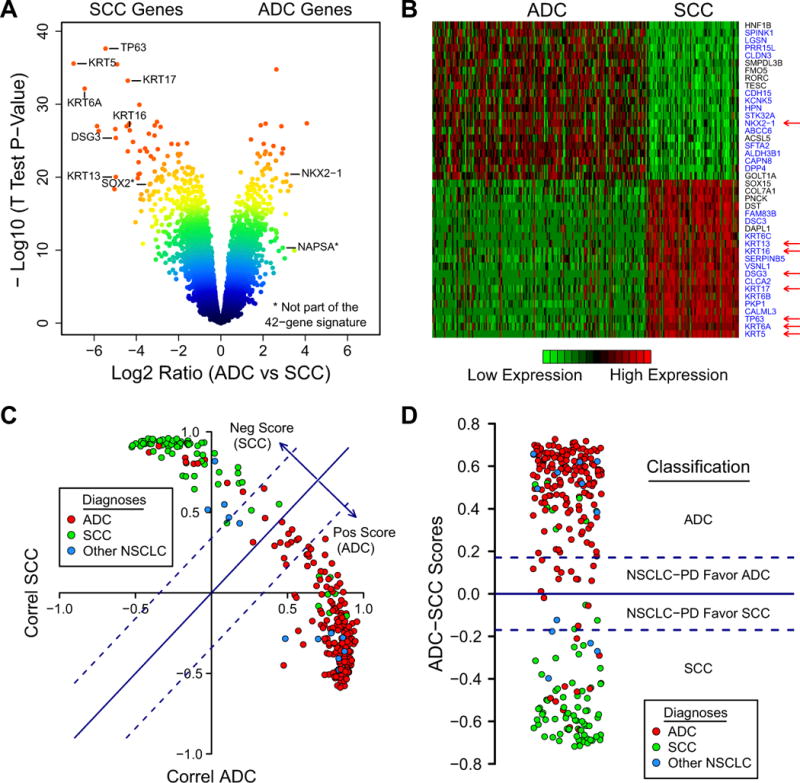
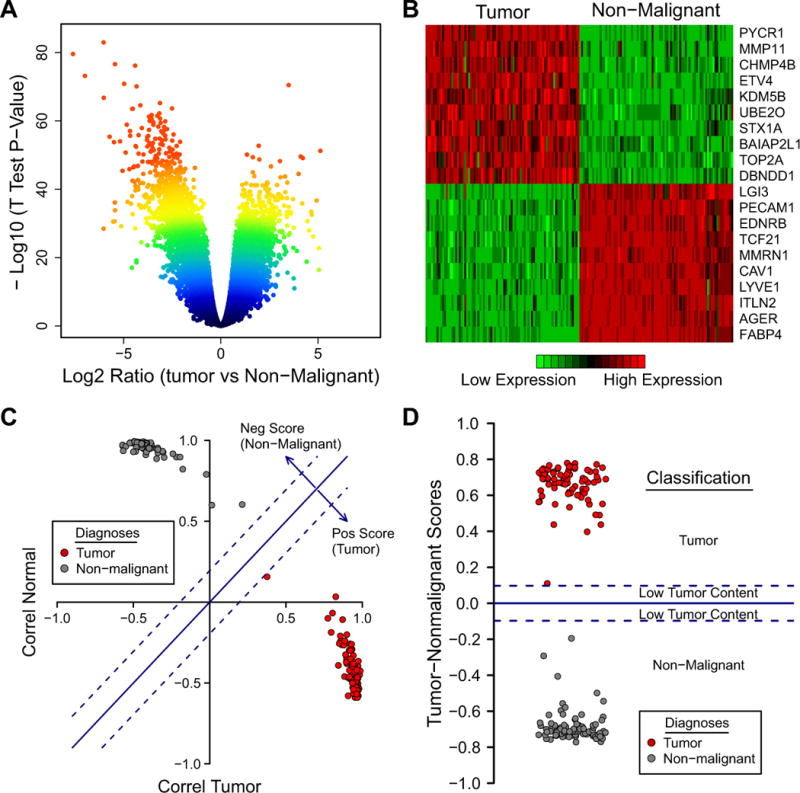
Experimental design: A microarray dataset of resected adenocarcinomas (ADC) and squamous cell carcinomas (SCC) was used as the learning set for an ADC-SCC signature. The Cancer Genome Atlas (TCGA) lung RNAseq dataset was used for validation. Another microarray dataset of ADCs and matched nonmalignant lung was used as the learning set for a tumor versus nonmalignant signature. The classifiers were selected as the most differentially expressed genes and sample classification was determined by a nearest distance approach.
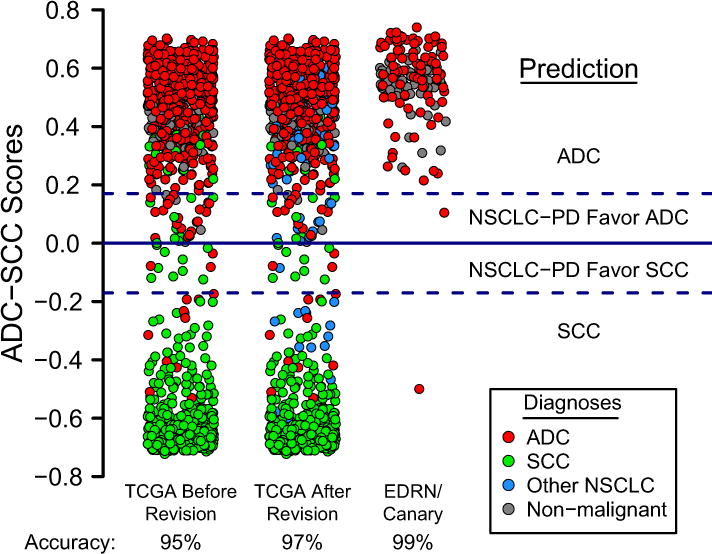
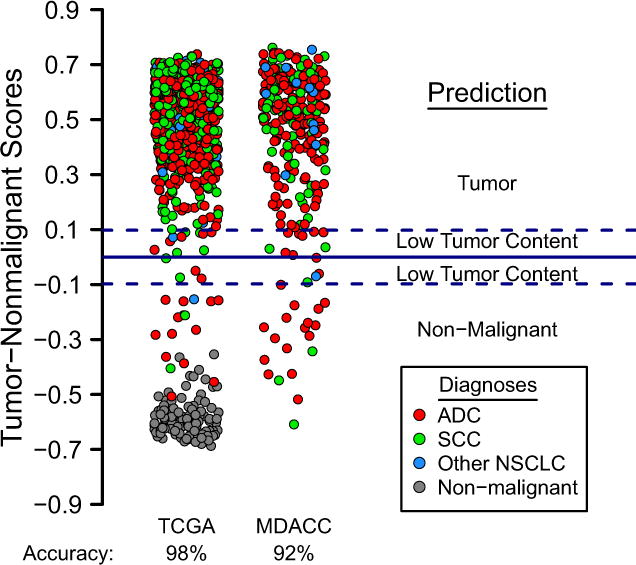
Results: We developed a 62-gene expression signature that contained many genes used in immunostains for NSCLC typing. It includes 42 genes that distinguish ADC from SCC and 20 genes differentiating nonmalignant lung from lung cancer. Testing of the TCGA and other public datasets resulted in high prediction accuracies (93%-95%). In addition, a prediction score was derived that correlates both with histologic grading and prognosis. We developed a practical version of the Classifier using the HTG EdgeSeq nuclease protection-based technology in combination with next-generation sequencing that can be applied to formalin-fixed paraffin-embedded (FFPE) tissues and small biopsies.
Conclusions: Our RNA classifier provides an objective, quantitative method to aid in the pathologic diagnosis of lung cancer. Clin Cancer Res; 22(19); 4880-9. ©2016 AACR.
©2016 American Association for Cancer Research.
Conflict of interest statement
Disclosure of Potential Conflicts of Interest: Ihab Botros and Debrah Thompson are both employees and stockholders of HTG Molecular Diagnostics, Inc. (HTG). Ignacio Wistuba is a consultant for HTG and an occasional participant of its advisory board. He also received financial support from HTG as part of a research agreement. No other authors of this article have financial ties to HTG.
Figures
References
-
- Travis W, Brambilla E, Burke A, Marx A, Nicholson A, editors. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4th. Lyon: International Agency for Research on Cancer; 2015. - PubMed
-
- Sun S, Schiller JH, Gazdar AF. Lung cancer in never smokers–a different disease. Nat Rev Cancer. 2007;7:778–90. - PubMed
-
- Rekhtman N, Tafe LJ, Chaft JE, Wang L, Arcila ME, Colanta A, et al. Distinct profile of driver mutations and clinical features in immunomarker-defined subsets of pulmonary large-cell carcinoma. Modern pathology : an official journal of the United States and Canadian Academy of Pathology, Inc. 2013;26:511–22. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
