

Endoscopy-Assisted Periacetabular Osteotomy
- PMID: 27354947
- PMCID: PMC4912685
- DOI: 10.1016/j.eats.2016.01.017
Endoscopy-Assisted Periacetabular Osteotomy
Abstract
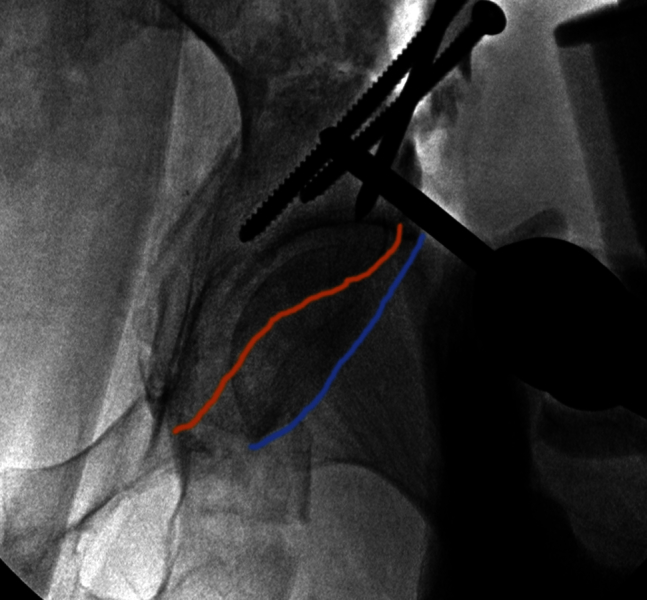
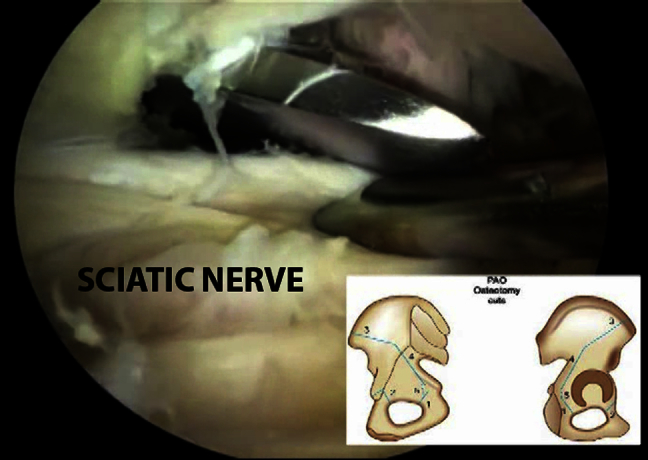
Minimizing soft tissue dissection and improving visualization of vital structures during periacetabular osteotomy (PAO) is of paramount importance to improve patient outcome and minimize complications. The endoscopy-assisted PAO was introduced to accomplish this objective. It involves an initial hip arthroscopy, for treatment of central compartment pathology, followed by a mini-open Bernese periacetabular osteotomy under fluoroscopic and endoscopic guidance, and completed by final dynamic hip arthroscopy to assess acetabular reorientation and fixation and to perform femoroplasty in relation to the new acetabular rim position, if needed. Endoscopy-assisted PAO is used to treat dysplasia or acetabular retroversion in a minimally invasive fashion.
Figures






References
-
- Ross J.R., Clohisy J.C., Baca G., Sink E., ANCHOR Investigators Patient and disease characteristics associated with hip arthroscopy failure in acetabular dysplasia. J Arthroplasty. 2014;29(9 suppl):160–163. - PubMed
-
- Matsuda D.K., Khatod M. Rapidly progressive osteoarthritis after arthroscopic labral repair in patients with hip dysplasia. Arthroscopy. 2012;28:1738–1743. - PubMed
-
- Fukui K., Briggs K.K., Trindade C.A., Philippon M.J. Outcomes after labral repair in patients with femoroacetabular impingement and borderline dysplasia. Arthroscopy. 2015;31:2371–2379. - PubMed
-
- Domb B.G., Stake C.E., Lindner D., El-Bitar Y., Jackson T.J. Arthroscopic capsular plication and labral preservation in borderline hip dysplasia: Two-year clinical outcomes of a surgical approach to a challenging problem. Am J Sports Med. 2013;41:2591–2598. - PubMed
-
- Ganz R., Klaue K., Vinh T.S., Mast J.W. A new periacetabular osteotomy for the treatment of hip dysplasias. Technique and preliminary results. Clin Orthop Relat Res. 1988;232:26–36. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
