

Hip Labral Reconstruction: The "Kite Technique" for Improved Efficiency and Graft Control
- PMID: 27354954
- PMCID: PMC4912620
- DOI: 10.1016/j.eats.2016.01.005
Hip Labral Reconstruction: The "Kite Technique" for Improved Efficiency and Graft Control
Abstract
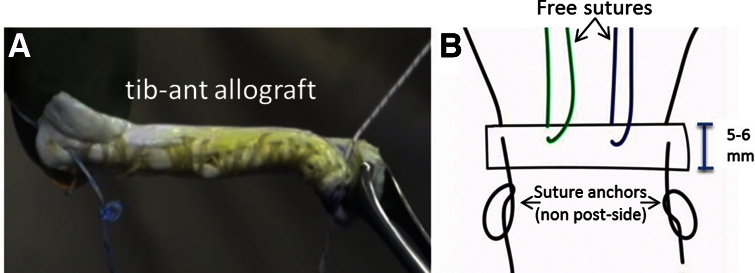
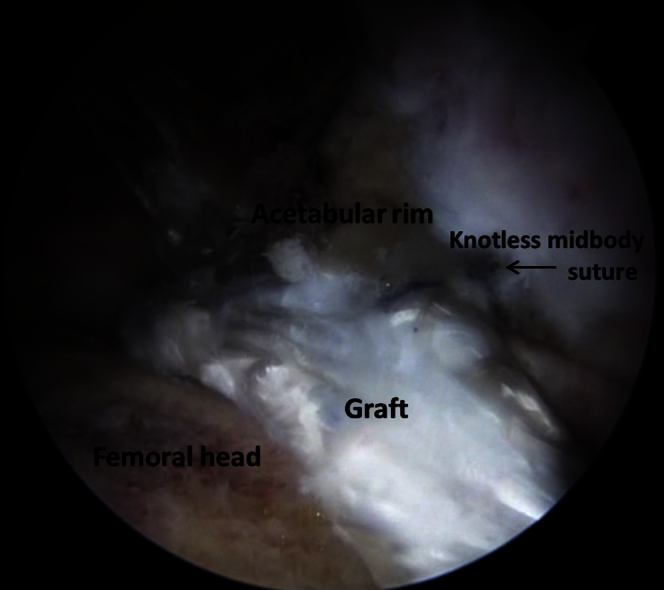
Although the merits of labral reconstruction have been well established, the technical difficulty of presently used reconstruction techniques-particularly with graft passage and fixation-limit its efficacy and potentiates the risk of iatrogenic damage within the hip joint. The unwieldy nature of a floating labral graft anchored on one end may impede accurate fixation of the other end, which is critical for restoration of the fluid hip seal and preservation of graft integrity. In this technique narrative, we present a "kite technique" for introduction, control, and efficient fixation of a labral reconstruction graft. The principles of this method are founded on the belief that a soft-tissue graft in an arthroscopic environment is much easier to guide into position with 2 control sutures using a pulley system similar to flying a kite with 2 fly lines. Although we herein detail the technique as it applies to labral reconstruction in the hip, the concept of the kite technique may also be employed in arthroscopic-assisted soft-tissue reconstructions of other joints.
Figures









References
-
- Bedi A., Kelly B.T., Khanduja V. Arthroscopic hip preservation surgery: Current concepts and perspective. Bone Joint J. 2013;95-B:10–19. - PubMed
-
- Philippon M.J., Nepple J.J., Campbell K.J. The hip fluid seal—Part I: The effect of an acetabular labral tear, repair, resection, and reconstruction on hip fluid pressurization. Knee Surg Sports Traumatol Arthrosc. 2014;22:722–729. - PubMed
-
- Nepple J.J., Philippon M.J., Campbell K.J. The hip fluid seal—Part II: The effect of an acetabular labral tear, repair, resection, and reconstruction on hip stability to distraction. Knee Surg Sports Traumatol Arthrosc. 2014;22:730–736. - PubMed
-
- Ferguson S.J., Bryant J.T., Ganz R., Ito K. An in vitro investigation of the acetabular labral seal in hip joint mechanics. J Biomech. 2003;36:171–178. - PubMed
-
- Espinosa N., Rothenfluh D.A., Beck M., Ganz R. Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am. 2006;88:925–935. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
