

The MRI features of placental adhesion disorder-a pictorial review
- PMID: 27355318
- PMCID: PMC5124928
- DOI: 10.1259/bjr.20160284
The MRI features of placental adhesion disorder-a pictorial review
Abstract
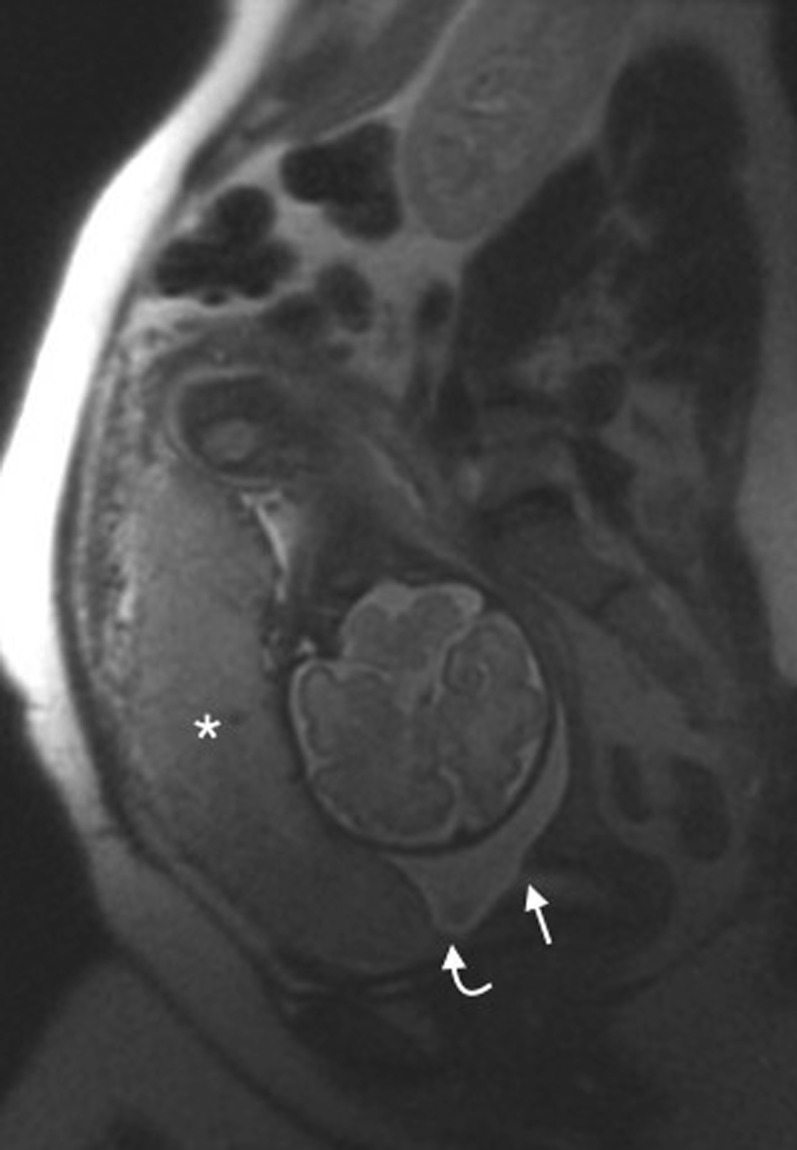
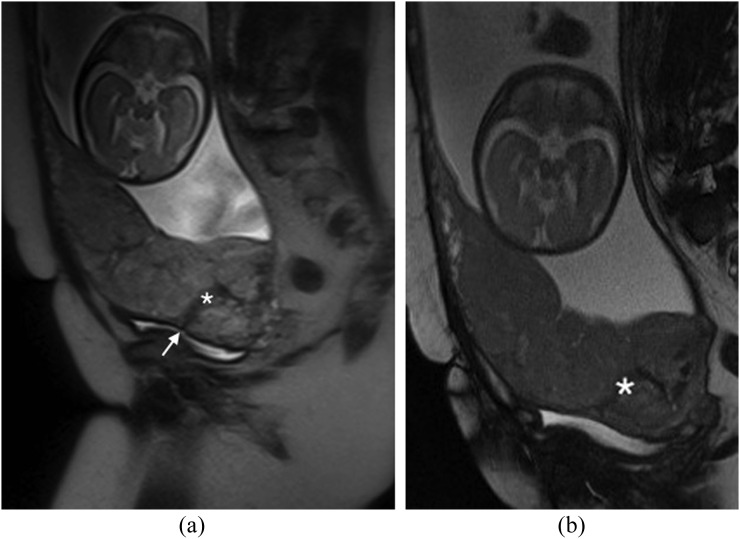
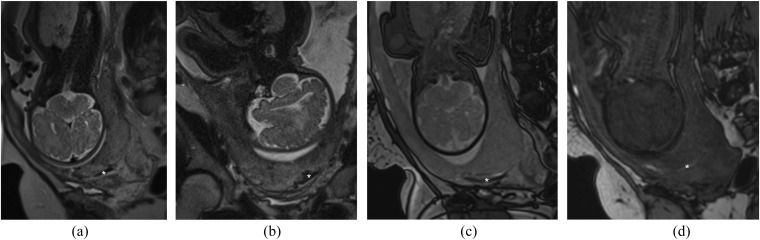
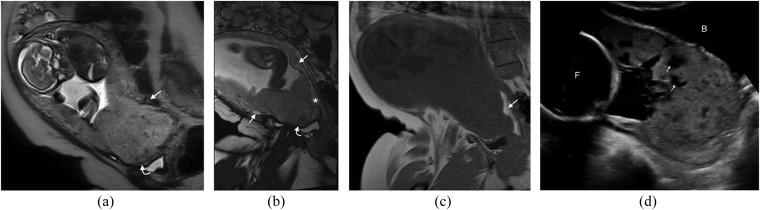
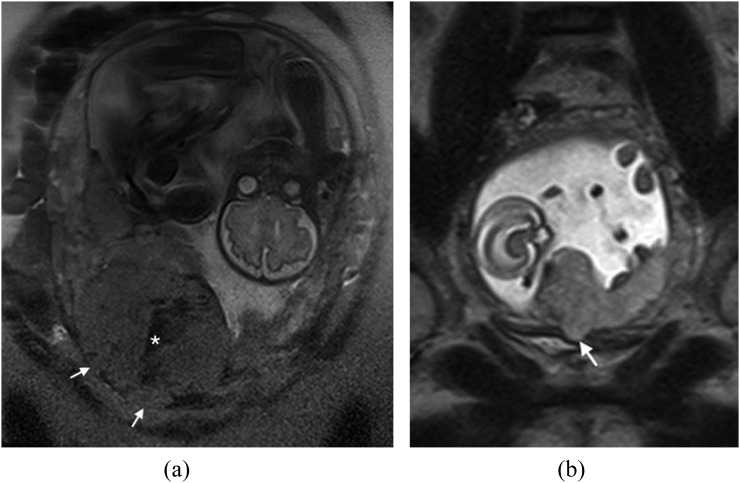
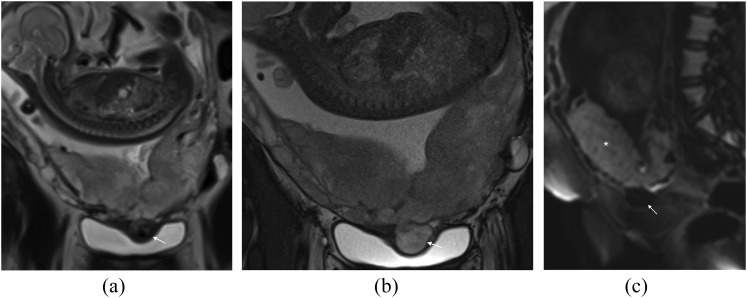
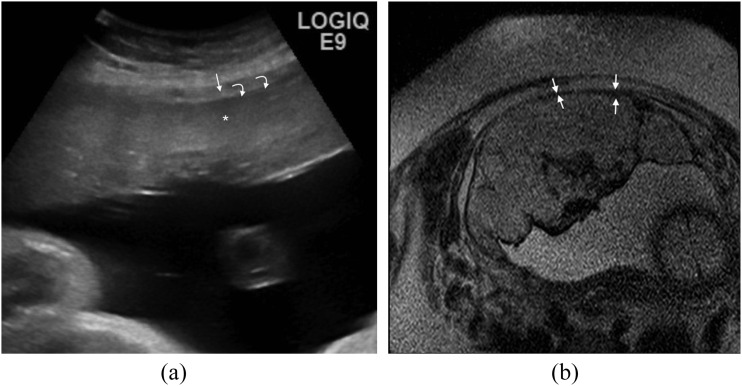
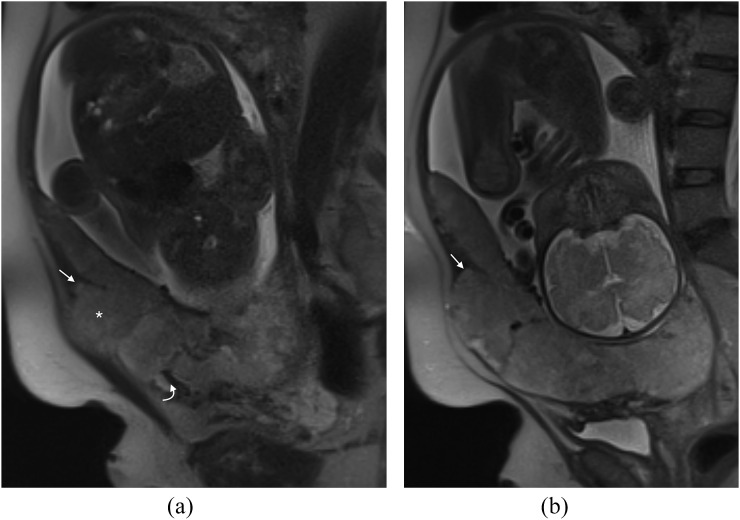
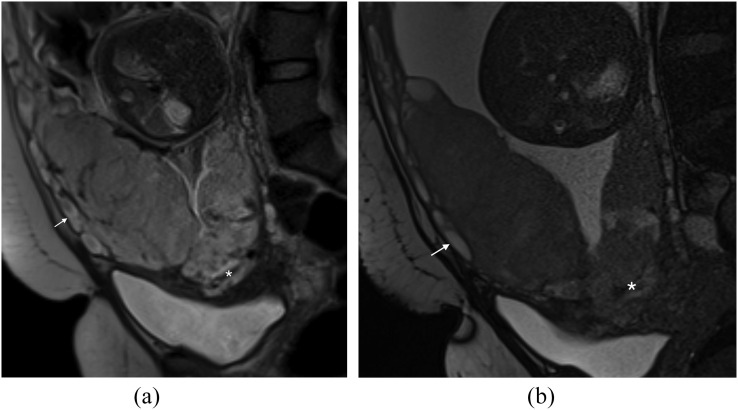
Placental adhesion disorder (PAD) comprises placenta accreta, increta and percreta lesions; these are classified according to the depth of uterine invasion. Although PAD is considered a rare condition, its incidence has increased 10-fold in the last 50 years. Ultrasound is the primary imaging modality for the assessment of the placenta and in the majority of cases, it is sufficient for diagnosis; however, when ultrasound findings are suspicious or inconclusive, MRI is recommended as an adjunct imaging technique. Numerous MRI features of PAD have been described, including dark intraplacental bands, disorganized intraplacental vascularity and abnormal uterine bulging. This pictorial review describes and illustrates these characteristics and discusses their implications in planning delivery. In addition, we present a series of "pitfall" cases to aid the interpreting radiologist and discuss management of PAD. PAD is a clinical and diagnostic challenge that is encountered with increasing frequency, requiring a cohesive multidisciplinary approach to its management.
Figures

Similar articles
-
Diagnostic accuracy of magnetic resonance imaging in assessing placental adhesion disorder in patients with placenta previa: Correlation with histological findings.Eur J Radiol. 2018 Sep;106:77-84. doi: 10.1016/j.ejrad.2018.07.014. Epub 2018 Jul 19. Eur J Radiol. 2018. PMID: 30150055
-
The value of specific MRI features in the evaluation of suspected placental invasion.Magn Reson Imaging. 2007 Jan;25(1):87-93. doi: 10.1016/j.mri.2006.10.007. Epub 2006 Nov 14. Magn Reson Imaging. 2007. PMID: 17222719
-
MRI of placental adhesive disorder.Br J Radiol. 2014 Oct;87(1042):20140294. doi: 10.1259/bjr.20140294. Epub 2014 Jul 25. Br J Radiol. 2014. PMID: 25060799 Free PMC article.
-
Placental evaluation with magnetic resonance.Radiol Clin North Am. 2013 Nov;51(6):955-66. doi: 10.1016/j.rcl.2013.07.009. Radiol Clin North Am. 2013. PMID: 24210438 Review.
-
Placenta accreta, increta, and percreta.Obstet Gynecol Clin North Am. 2013 Mar;40(1):137-54. doi: 10.1016/j.ogc.2012.12.002. Obstet Gynecol Clin North Am. 2013. PMID: 23466142 Review.
Cited by
-
Placental magnetic resonance imaging: normal appearance, anatomical variations, and pathological findings.Radiol Bras. 2021 Mar-Apr;54(2):123-129. doi: 10.1590/0100-3984.2020.0010. Radiol Bras. 2021. PMID: 33854267 Free PMC article.
-
Magnetic resonance imaging of the female pelvis after Cesarean section: a pictorial review.Insights Imaging. 2020 May 27;11(1):75. doi: 10.1186/s13244-020-00876-5. Insights Imaging. 2020. PMID: 32462368 Free PMC article. Review.
-
Placental volume as a novel sign for identifying placenta accreta spectrum in pregnancies with complete placenta previa.BMC Pregnancy Childbirth. 2024 Jan 10;24(1):52. doi: 10.1186/s12884-024-06247-y. BMC Pregnancy Childbirth. 2024. PMID: 38200440 Free PMC article.
-
The haemodynamics of the human placenta in utero.PLoS Biol. 2020 May 28;18(5):e3000676. doi: 10.1371/journal.pbio.3000676. eCollection 2020 May. PLoS Biol. 2020. PMID: 32463837 Free PMC article.
-
Role of scaling combination of risk factors in clinical and imaging findings during pregnancy in predicting placenta accreta spectrum.Caspian J Intern Med. 2022 Winter;13(1):10-15. doi: 10.22088/cjim.13.1.10. Caspian J Intern Med. 2022. PMID: 35178202 Free PMC article.
References
-
- Placenta Praevia, Placenta Praevia Accreta and Vasa Praevia: Diagnosis and Management. RCOG (Green-top guideline No. 27). Internet; 2011; 4.6.
-
- NICE, Caesarean Section, in CG132; 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
