

Impact of Weight Extremes on Clinical Outcomes in Pediatric Acute Respiratory Distress Syndrome
- PMID: 27355525
- PMCID: PMC5199718
- DOI: 10.1097/CCM.0000000000001857
Impact of Weight Extremes on Clinical Outcomes in Pediatric Acute Respiratory Distress Syndrome
Abstract
Objectives: To determine whether weight extremes impact clinical outcomes in pediatric acute respiratory distress syndrome.
Design: Post hoc analysis of a cohort created by combining five multicenter pediatric acute respiratory distress syndrome studies.
Setting: Forty-three academic PICUs worldwide.
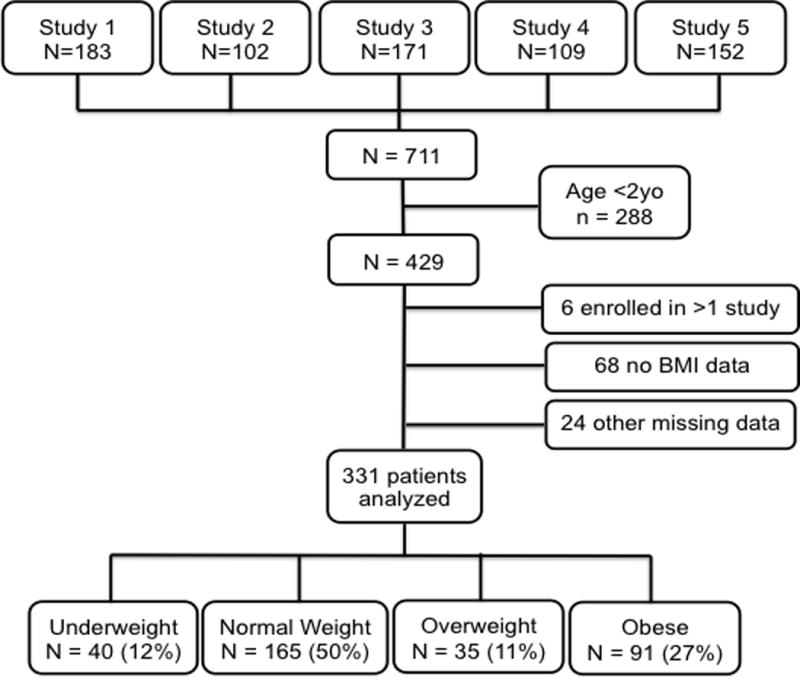
Patients: A total of 711 subjects prospectively diagnosed with pediatric acute respiratory distress syndrome.
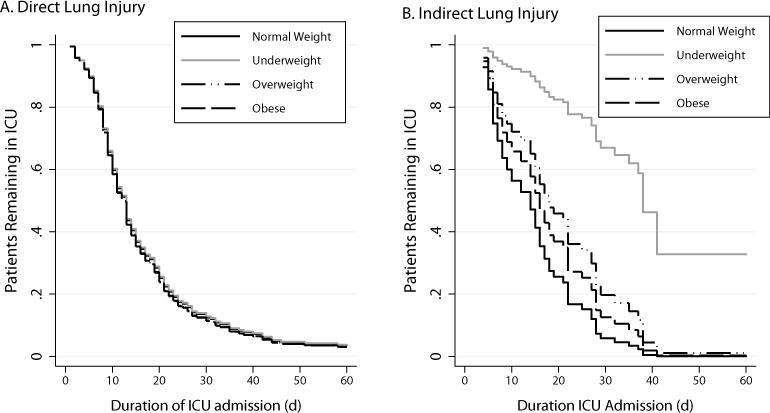
Intervention: Subjects more than 2 years were included and categorized by Center for Disease Control and Prevention body mass index z score criteria: underweight (< -1.89), normal weight (-1.89 to +1.04), overweight (+1.05 to +1.64), and obese (≥ +1.65). Subjects were stratified by direct versus indirect lung injury leading to pediatric acute respiratory distress syndrome. The primary outcome was in-hospital mortality. In survivors, secondary analyses included duration of mechanical ventilation and ICU length of stay.
Measurements and main results: A total of 331 patients met inclusion criteria; 12% were underweight, 50% normal weight, 11% overweight, and 27% obese. Overall mortality was 20%. By multivariate analysis, body mass index category was independently associated with mortality (p = 0.004). When stratified by lung injury type, there was no mortality difference between body mass index groups with direct lung injury; however, in the indirect lung injury group, the odds of mortality in the obese were significantly lower than normal weight subjects (odds ratio, 0.11; 95% CI, 0.02-0.84). Survivors with direct lung injury had no difference in the duration of mechanical ventilation or ICU length of stay; however, those with indirect lung injury, the overweight required longer duration of mechanical ventilation than other groups (p < 0.001).
Conclusions: These data support the obesity paradox in pediatric acute respiratory distress syndrome. Obese children with indirect lung injury pediatric acute respiratory distress syndrome have a lower risk of mortality. Importantly, among survivors, the overweight with indirect lung injury requires longer duration of mechanical ventilation. Our data require prospective validation to further elucidate the pathobiology of this phenomenon.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

Comment in
-
Nutritional Assessment Must be Prioritized for Critically Ill Children in the PICU.Crit Care Med. 2017 Apr;45(4):e464. doi: 10.1097/CCM.0000000000002220. Crit Care Med. 2017. PMID: 28291114 No abstract available.
-
The authors reply.Crit Care Med. 2017 Apr;45(4):e464-e465. doi: 10.1097/CCM.0000000000002276. Crit Care Med. 2017. PMID: 28291115 Free PMC article. No abstract available.
-
Is the Obesity Paradox Valid in Pediatric Intensive Care?Crit Care Med. 2017 May;45(5):e536-e537. doi: 10.1097/CCM.0000000000002329. Crit Care Med. 2017. PMID: 28410325 No abstract available.
-
The authors reply.Crit Care Med. 2017 May;45(5):e537-e538. doi: 10.1097/CCM.0000000000002356. Crit Care Med. 2017. PMID: 28410326 Free PMC article. No abstract available.
References
-
- Fryar, MSPH Cheryl D, Ogden, PhD Cynthia L. D of H and NE, Surveys: Prevalence of Underweight Among Adults Aged 20 Years and Over: United States, 2007–2008. 2010
-
- Ogden CL, Carroll MD, Kit BK, et al. Prevalence of obesity in the United States, 2009–2010. NCHS Data Brief. 2012:1–8. - PubMed
-
- Pieracci FM, Hydo L, Pomp A, et al. The relationship between body mass index and postoperative mortality from critical illness. Obes Surg. 2008;18:501–7. - PubMed
-
- Newell Ma, Bard MR, Goettler CE, et al. Body mass index and outcomes in critically injured blunt trauma patients: weighing the impact. J Am Coll Surg. 2007;204:1056–61. discussion 1062–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
