

Randomized Trial of Video Laryngoscopy for Endotracheal Intubation of Critically Ill Adults
- PMID: 27355526
- PMCID: PMC5203695
- DOI: 10.1097/CCM.0000000000001841
Randomized Trial of Video Laryngoscopy for Endotracheal Intubation of Critically Ill Adults
Abstract
Objective: To evaluate the effect of video laryngoscopy on the rate of endotracheal intubation on first laryngoscopy attempt among critically ill adults.
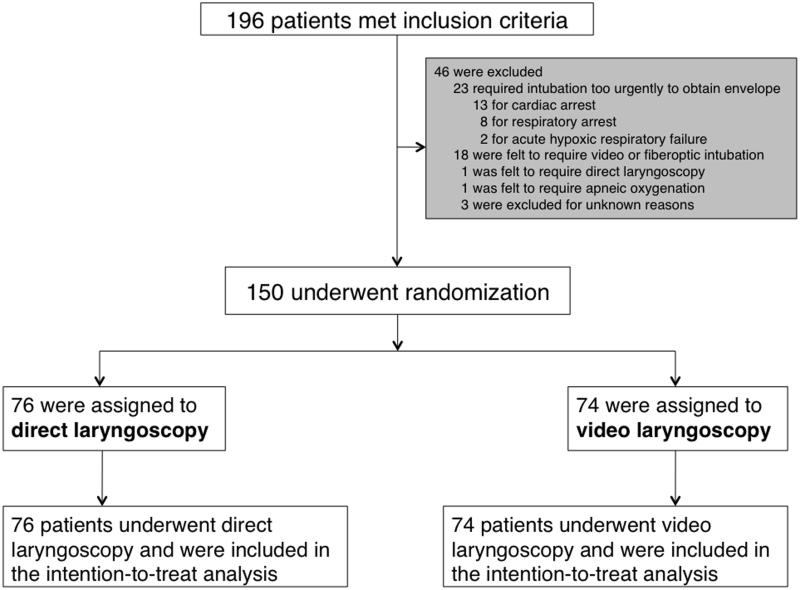
Design: A randomized, parallel-group, pragmatic trial of video compared with direct laryngoscopy for 150 adults undergoing endotracheal intubation by Pulmonary and Critical Care Medicine fellows.
Setting: Medical ICU in a tertiary, academic medical center.
Patients: Critically ill patients 18 years old or older.
Interventions: Patients were randomized 1:1 to video or direct laryngoscopy for the first attempt at endotracheal intubation.
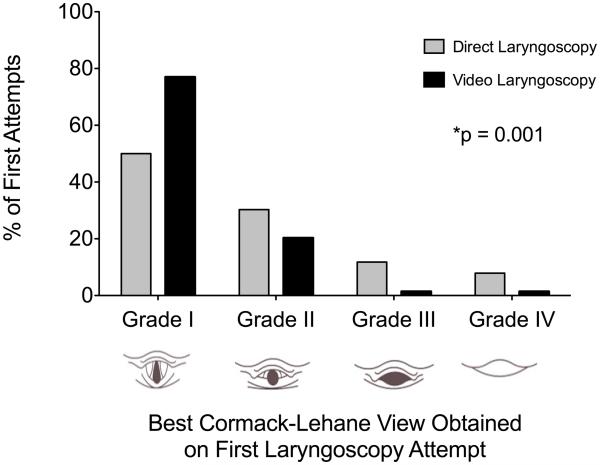
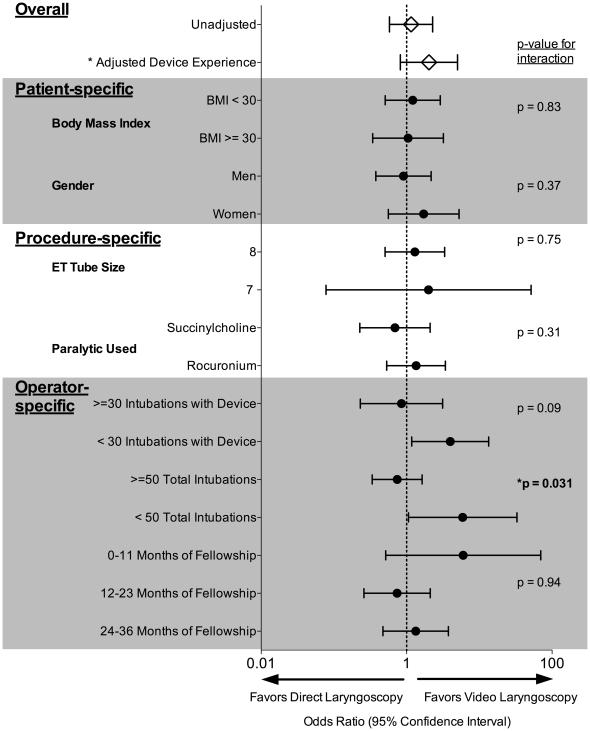
Measurements and main results: Patients assigned to video (n = 74) and direct (n = 76) laryngoscopy were similar at baseline. Despite better glottic visualization with video laryngoscopy, there was no difference in the primary outcome of intubation on the first laryngoscopy attempt (video 68.9% vs direct 65.8%; p = 0.68) in unadjusted analyses or after adjustment for the operator's previous experience with the assigned device (odds ratio for video laryngoscopy on intubation on first attempt 2.02; 95% CI, 0.82-5.02, p = 0.12). Secondary outcomes of time to intubation, lowest arterial oxygen saturation, complications, and in-hospital mortality were not different between video and direct laryngoscopy.
Conclusions: In critically ill adults undergoing endotracheal intubation, video laryngoscopy improves glottic visualization but does not appear to increase procedural success or decrease complications.
Figures
Comment in
-
Video Laryngoscopy Versus Direct Laryngoscopy in the ICU: Don't Throw Away That MAC Blade Just Yet.Crit Care Med. 2016 Nov;44(11):2106-2107. doi: 10.1097/CCM.0000000000001924. Crit Care Med. 2016. PMID: 27755070 No abstract available.
-
Comparing Video and Direct Laryngoscopy in Critically Ill Patients: Rational Study Design Is Important.Crit Care Med. 2017 Mar;45(3):e326. doi: 10.1097/CCM.0000000000002191. Crit Care Med. 2017. PMID: 28212227 No abstract available.
-
The authors reply.Crit Care Med. 2017 Mar;45(3):e326-e327. doi: 10.1097/CCM.0000000000002216. Crit Care Med. 2017. PMID: 28212228 Free PMC article. No abstract available.
-
Randomized Trial of Video Laryngoscopy for Endotracheal Intubation of Critically Ill Adults: More Data, More Questions.Crit Care Med. 2017 Apr;45(4):e460-e461. doi: 10.1097/CCM.0000000000002218. Crit Care Med. 2017. PMID: 28291110 No abstract available.
-
The authors reply.Crit Care Med. 2017 Apr;45(4):e461. doi: 10.1097/CCM.0000000000002271. Crit Care Med. 2017. PMID: 28291111 Free PMC article. No abstract available.
-
Video Laryngoscopy for Endotracheal Intubation of Critically Ill Adults-Role of Different Blades and Stylets.Crit Care Med. 2017 Apr;45(4):e461-e463. doi: 10.1097/CCM.0000000000002231. Crit Care Med. 2017. PMID: 28291112 No abstract available.
-
The authors reply.Crit Care Med. 2017 Apr;45(4):e463. doi: 10.1097/CCM.0000000000002270. Crit Care Med. 2017. PMID: 28291113 Free PMC article. No abstract available.
References
-
- Jaber S, Jung B, Corne P, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med. 2010;36:248–255. - PubMed
-
- Cook TM, Woodall N, Harper J, et al. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: intensive care and emergency departments. Br J Anaesth. 2011;106:632–642. - PubMed
-
- Simpson GD, Ross MJ, McKeown DW, et al. Tracheal intubation in the critically ill: a multi-centre national study of practice and complications. Br J Anaesth. 2012;108:792–799. - PubMed
-
- Mort TC. The incidence and risk factors for cardiac arrest during emergency tracheal intubation: a justification for incorporating the ASA Guidelines in the remote location. J Clin Anesth. 2004;16:508–516. - PubMed
-
- Jabre P, Combes X, Lapostolle F, et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet. 2009;374:293–300. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
