

Utility of CSF biomarkers in psychiatric disorders: a national multicentre prospective study
- PMID: 27357952
- PMCID: PMC4928321
- DOI: 10.1186/s13195-016-0192-z
Utility of CSF biomarkers in psychiatric disorders: a national multicentre prospective study
Abstract
Background: Affective and psychotic disorders are mental or behavioural patterns resulting in an inability to cope with life's ordinary demands and routines. These conditions can be a prodromal event of Alzheimer's disease (AD). The prevalence of underlying AD lesions in psychiatric diseases is unknown, and it would be helpful to determine them in patients. AD cerebrospinal fluid (CSF) biomarkers (amyloid β, tau and phosphorylated tau) have high diagnostic accuracy, both for AD with dementia and to predict incipient AD (mild cognitive impairment due to AD), and they are sometimes used to discriminate psychiatric diseases from AD. Our objective in the present study was to evaluate the clinical utility of CSF biomarkers in a group of patients with psychiatric disease as the main diagnosis.
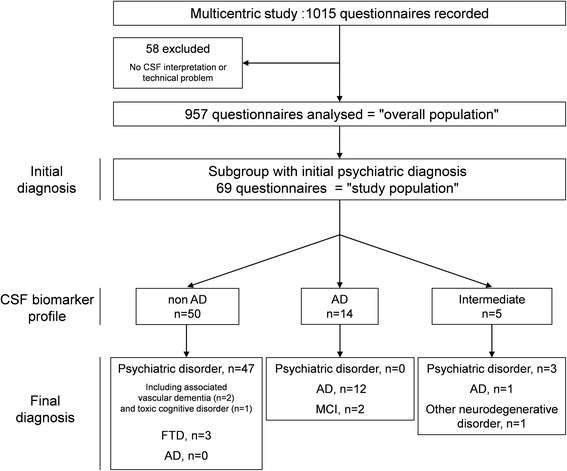
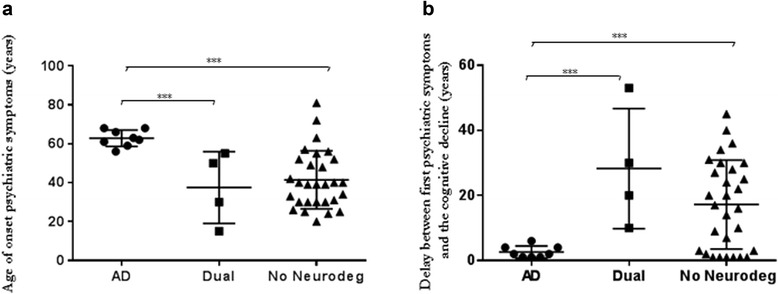
Methods: In a multicentre prospective study, clinicians filled out an anonymous questionnaire about all of their patients who had undergone CSF biomarker evaluation. Before and after CSF biomarker results were obtained, clinicians provided a diagnosis with their level of confidence and information about the treatment. We included patients with a psychiatric disorder as the initial diagnosis. In a second part of the study conducted retrospectively in a followed subgroup, clinicians detailed the psychiatric history and we classified patients into three categories: (1) psychiatric symptoms associated with AD, (2) dual diagnosis and (3) cognitive decline not linked to a neurodegenerative disorder.
Results: Of 957 patients, 69 had an initial diagnosis of a psychiatric disorder. Among these 69 patients, 14 (20.2 %) had a CSF AD profile, 5 (7.2 %) presented with an intermediate CSF profile and 50 (72.4 %) had a non-AD CSF profile. Ultimately, 13 (18.8 %) patients were diagnosed with AD. We show that in the AD group psychiatric symptoms occurred later and the delay between the first psychiatric symptoms and the cognitive decline was shorter.
Conclusions: This study revealed that about 20 % of patients with a primary psychiatric disorder diagnosis before undergoing a CSF exploration for cognitive disorder displayed a CSF biomarker AD profile. In memory clinics, it seems important to consider AD as a possible diagnosis before finalizing a diagnosis of a psychiatric disorder.
Keywords: Alzheimer’s disease; Biomarkers; Cerebrospinal fluid; Clinical practice; Psychiatric disease.
Figures
References
-
- Albert MS, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–9. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
