

Neuropathological criteria of anti-IgLON5-related tauopathy
- PMID: 27358064
- PMCID: PMC5023728
- DOI: 10.1007/s00401-016-1591-8
Neuropathological criteria of anti-IgLON5-related tauopathy
Abstract
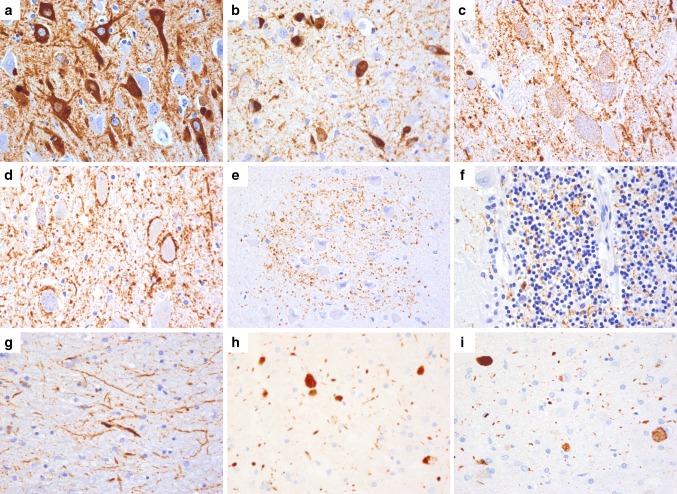
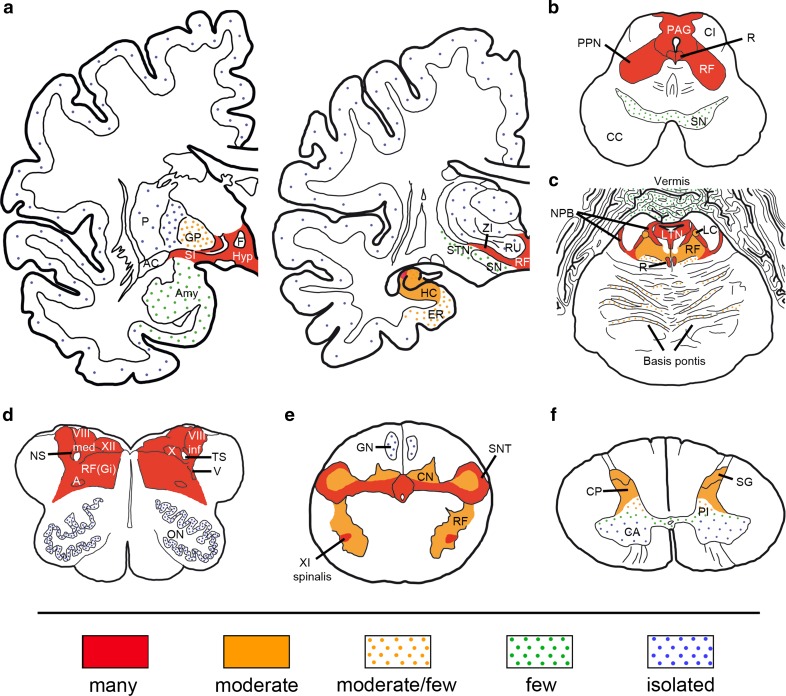
We recently reported a novel neurological syndrome characterized by a unique NREM and REM parasomnia with sleep apnea and stridor, accompanied by bulbar dysfunction and specific association with antibodies against the neuronal cell-adhesion protein IgLON5. All patients had the HLA-DRB1*1001 and HLA-DQB1*0501 alleles. Neuropathological findings in two patients revealed a novel tauopathy restricted to neurons and predominantly involving the hypothalamus and tegmentum of the brainstem. The aim of the current study is to describe the neuropathological features of the anti-IgLON5 syndrome and to provide diagnostic levels of certainty based on the presence of associated clinical and immunological data. The brains of six patients were examined and the features required for the neuropathological diagnosis were established by consensus. Additional clinical and immunological criteria were used to define "definite", "probable" and "possible" diagnostic categories. The brains of all patients showed remarkably similar features consistent with a neurodegenerative disease with neuronal loss and gliosis and absence of inflammatory infiltrates. The most relevant finding was the neuronal accumulation of hyperphosphorylated tau composed of both three-repeat (3R) and four-repeat (4R) tau isoforms, preferentially involving the hypothalamus, and more severely the tegmental nuclei of the brainstem with a cranio-caudal gradient of severity until the upper cervical cord. A "definite" diagnosis of anti-IgLON5-related tauopathy is established when these neuropathological features are present along with the detection of serum or CSF IgLON5 antibodies. When the antibody status is unknown, a "probable" diagnosis requires neuropathological findings along with a compatible clinical history or confirmation of possession of HLA-DRB1*1001 and HLA-DQB1*0501 alleles. A "possible" diagnosis should be considered in cases with compatible neuropathology but without information about a relevant clinical presentation and immunological status. These criteria should help to identify undiagnosed cases among archival tissue, and will assist future clinicopathological studies of this novel disorder.
Keywords: Brainstem; IgLON5; NREM; Parasomnia; Tauopathy.
Conflict of interest statement
Compliance with ethical standardsFundingThis study was partly supported by grants from Fundació Marató de TV3 to EG (grant no. 20141610), Fondo de Investigaciones Sanitarias, FEDER, (FIS 15/00377, FG), (FIS 14/00203, JD) and CIBERER (JD), Madrid, Spain, Fundació CELLEX (JD), and NIH RO1NS077851 (JD).DisclosuresJD receives royalties from licensing fees to Athena diagnostics for a patent for the use of Ma2 and autoantibody test, and from licensing fees to Euroimmun for patents for the use of NMDAR and GABAbR as autoantibody tests, and licensing fees for the use of DPPX, GABAaR, and IgLON5 antibodies as diagnostic tests. JD has received a research grant from Euroimmun. FG receives royalties from licensing fees to Euroimmun for the use of IgLON5 as a diagnostic test.Conflict of interestEG, RH, HL, JH, TD, MP, JP, BH, GR, JS, HB, TR, GK declare that they have no conflict of interest.
Figures

References
-
- Dickson DW, Hauw JJ, Agid Y, Litvan I. Progressive supranuclear palsy and corticobasal degeneration. In: Dickson DW, Weller RO, editors. Neurodegeneration: the molecular pathology of dementia and movement disorders. 2. New York: Wiley–Blackwell Publishers; 2011. pp. 135–155.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
