

Long-Term Risk of Atherosclerotic Cardiovascular Disease in US Adults With the Familial Hypercholesterolemia Phenotype
- PMID: 27358432
- PMCID: PMC4933328
- DOI: 10.1161/CIRCULATIONAHA.116.022335
Long-Term Risk of Atherosclerotic Cardiovascular Disease in US Adults With the Familial Hypercholesterolemia Phenotype
Abstract
Background: Heterozygous familial hypercholesterolemia (FH) affects up to 1 in 200 individuals in the United States, but atherosclerotic cardiovascular disease (ASCVD) outcomes of FH in the general US population have not been described. We therefore sought to evaluate long-term coronary heart disease (CHD) and total ASCVD risks in US adults with an FH phenotype.
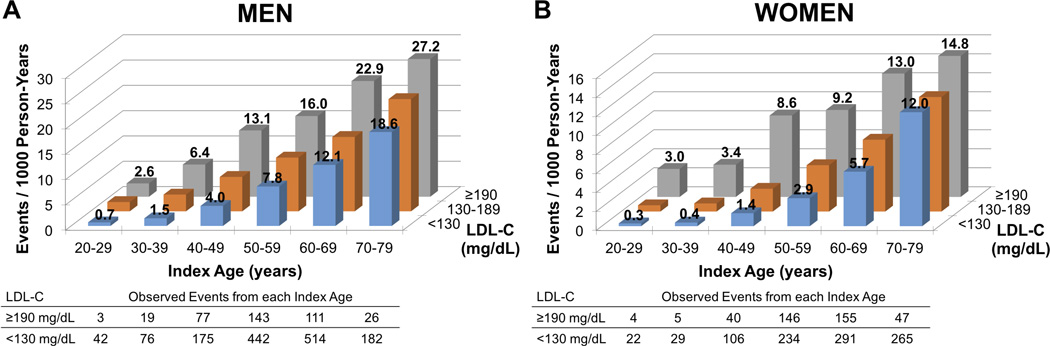
Methods: Using individual pooled data from 6 large US epidemiological cohorts, we stratified participants by low-density lipoprotein cholesterol level at index ages from 20 to 79 years. For the primary analysis, low-density lipoprotein cholesterol levels ≥190 and <130 mg/dL defined the FH phenotype and referent, respectively. Sensitivity analyses evaluated the effects of varying the FH phenotype definition. We used Cox regression models to assess covariate-adjusted associations of the FH phenotype with 30-year hazards for CHD (CHD death or nonfatal myocardial infarction) and total ASCVD (CHD or stroke).
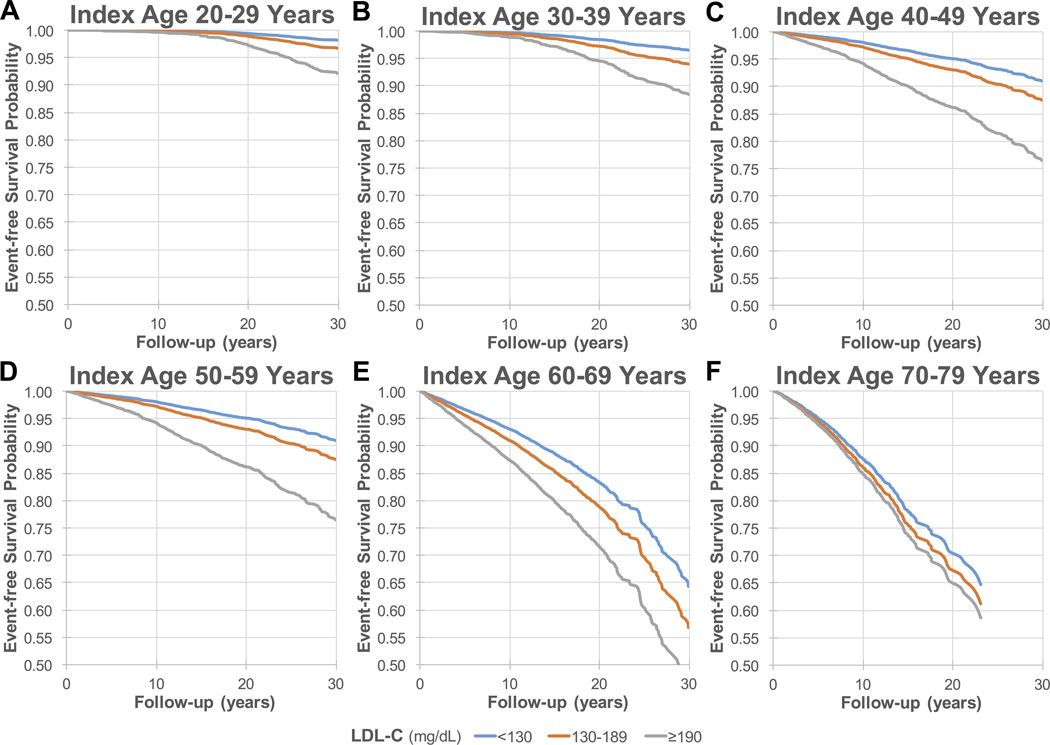
Results: We included 68 565 baseline person-examinations; 3850 (5.6%) had the FH phenotype by the primary definition. Follow-up across index ages ranged from 78 985 to 308 378 person-years. After covariate adjustment, the FH phenotype was associated with substantially elevated 30-year CHD risk, with hazard ratios up to 5.0 (95% confidence interval, 1.1-21.7). Across index ages, CHD risk was accelerated in those with the FH phenotype by 10 to 20 years in men and 20 to 30 years in women. Similar patterns of results were found for total ASCVD risk, with hazard ratios up to 4.1 (95% confidence interval, 1.2-13.4). Alternative FH phenotype definitions incorporating family history, more stringent age-based low-density lipoprotein cholesterol thresholds, or alternative lipid fractions decreased the FH phenotype prevalence to as low as 0.2% to 0.4% without materially affecting CHD risk estimates (hazard ratios up to 8.0; 95% confidence interval, 1.0-61.6).
Conclusions: In the general US population, the long-term ASCVD burden related to phenotypic FH, defined by low-density lipoprotein cholesterol ≥190 mg/dL, is likely substantial. Our finding of CHD risk acceleration may aid efforts in risk communication.
Keywords: coronary disease; epidemiology; hypercholesterolemia.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Enough Evidence, Time to Act!Circulation. 2016 Jul 5;134(1):20-3. doi: 10.1161/CIRCULATIONAHA.116.023010. Circulation. 2016. PMID: 27358433 No abstract available.
References
-
- de Ferranti SD, Rodday AM, Mendelson MM, Wong JB, Leslie LK, Sheldrick RC. Prevalence of familial hypercholesterolemia in the 1999 to 2012 United States National Health and Nutrition Examination Surveys (NHANES) Circulation. 2016;133:1067–1072. - PubMed
-
- Do R, Stitziel NO, Won HH, Jorgensen AB, Duga S, Angelica Merlini P, Kiezun A, Farrall M, Goel A, Zuk O, Guella I, Asselta R, Lange LA, Peloso GM, Auer PL, Girelli D, Martinelli N, Farlow DN, DePristo MA, Roberts R, Stewart AF, Saleheen D, Danesh J, Epstein SE, Sivapalaratnam S, Hovingh GK, Kastelein JJ, Samani NJ, Schunkert H, Erdmann J, Shah SH, Kraus WE, Davies R, Nikpay M, Johansen CT, Wang J, Hegele RA, Hechter E, Marz W, Kleber ME, Huang J, Johnson AD, Li M, Burke GL, Gross M, Liu Y, Assimes TL, Heiss G, Lange EM, Folsom AR, Taylor HA, Olivieri O, Hamsten A, Clarke R, Reilly DF, Yin W, Rivas MA, Donnelly P, Rossouw JE, Psaty BM, Herrington DM, Wilson JG, Rich SS, Bamshad MJ, Tracy RP, Cupples LA, Rader DJ, Reilly MP, Spertus JA, Cresci S, Hartiala J, Tang WH, Hazen SL, Allayee H, Reiner AP, Carlson CS, Kooperberg C, Jackson RD, Boerwinkle E, Lander ES, Schwartz SM, Siscovick DS, McPherson R, Tybjaerg-Hansen A, Abecasis GR, Watkins H, Nickerson DA, Ardissino D, Sunyaev SR, O'Donnell CJ, Altshuler D, Gabriel S, Kathiresan S. Exome sequencing identifies rare LDLR and APOA5 alleles conferring risk for myocardial infarction. Nature. 2015;518:102–106. - PMC - PubMed
-
- Scientific Steering Committee, Simon Broome Register Group. Mortality in treated heterozygous familial hypercholesterolaemia. Atherosclerosis. 1999;142:105–112. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
