

Phenotype-Specific Treatment of Heart Failure With Preserved Ejection Fraction: A Multiorgan Roadmap
- PMID: 27358439
- PMCID: PMC4930115
- DOI: 10.1161/CIRCULATIONAHA.116.021884
Phenotype-Specific Treatment of Heart Failure With Preserved Ejection Fraction: A Multiorgan Roadmap
Abstract
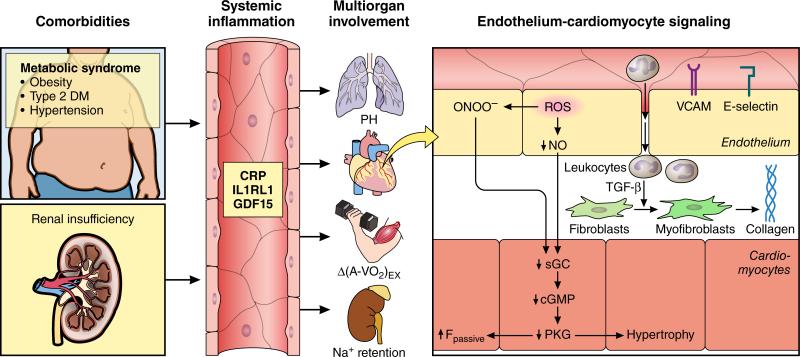
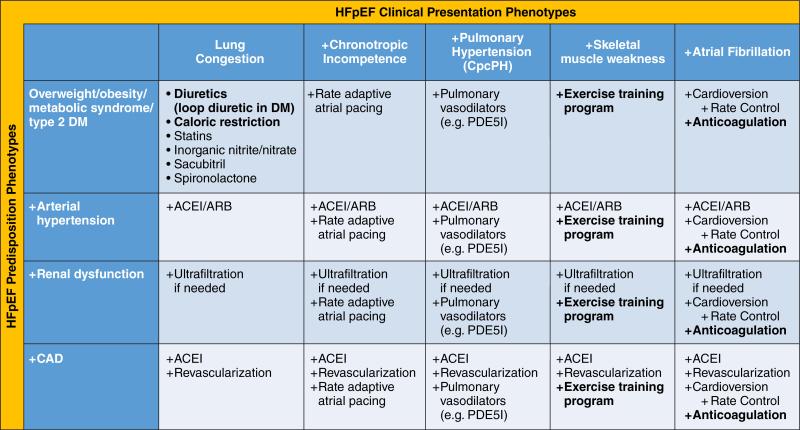
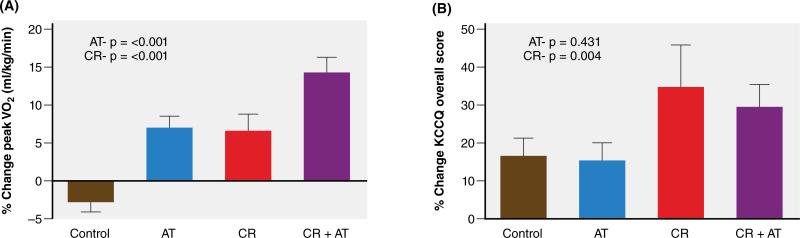
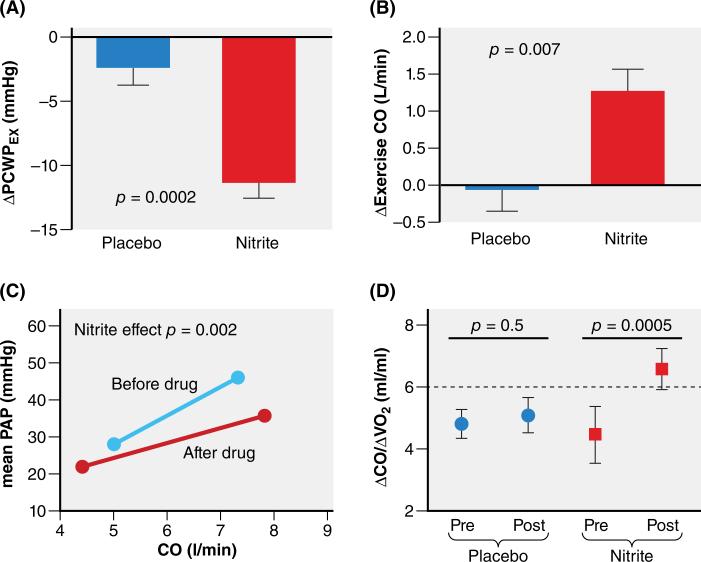
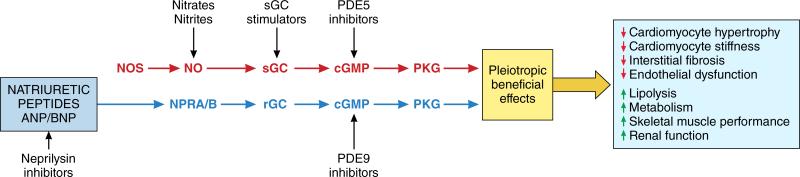
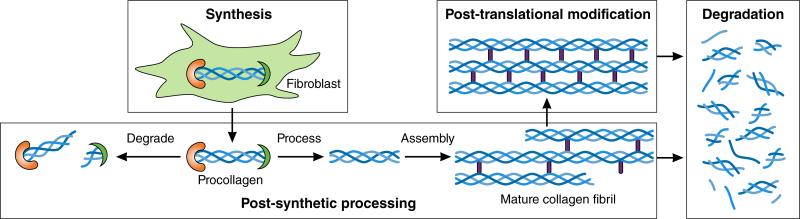
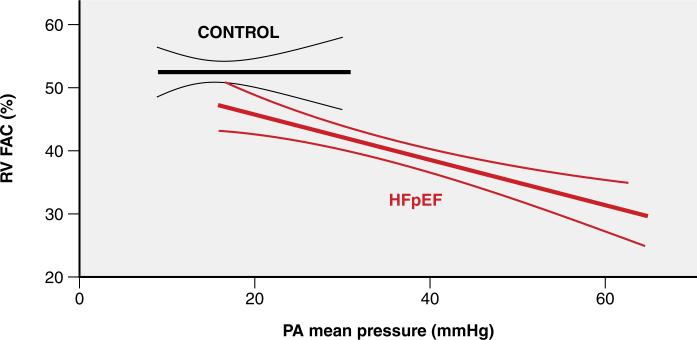
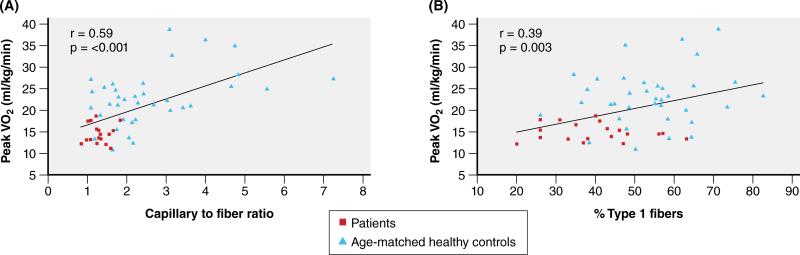
Heart failure (HF) with preserved ejection fraction (EF; HFpEF) accounts for 50% of HF cases, and its prevalence relative to HF with reduced EF continues to rise. In contrast to HF with reduced EF, large trials testing neurohumoral inhibition in HFpEF failed to reach a positive outcome. This failure was recently attributed to distinct systemic and myocardial signaling in HFpEF and to diversity of HFpEF phenotypes. In this review, an HFpEF treatment strategy is proposed that addresses HFpEF-specific signaling and phenotypic diversity. In HFpEF, extracardiac comorbidities such as metabolic risk, arterial hypertension, and renal insufficiency drive left ventricular remodeling and dysfunction through systemic inflammation and coronary microvascular endothelial dysfunction. The latter affects left ventricular diastolic dysfunction through macrophage infiltration, resulting in interstitial fibrosis, and through altered paracrine signaling to cardiomyocytes, which become hypertrophied and stiff because of low nitric oxide and cyclic guanosine monophosphate. Systemic inflammation also affects other organs such as lungs, skeletal muscle, and kidneys, leading, respectively, to pulmonary hypertension, muscle weakness, and sodium retention. Individual steps of these signaling cascades can be targeted by specific interventions: metabolic risk by caloric restriction, systemic inflammation by statins, pulmonary hypertension by phosphodiesterase 5 inhibitors, muscle weakness by exercise training, sodium retention by diuretics and monitoring devices, myocardial nitric oxide bioavailability by inorganic nitrate-nitrite, myocardial cyclic guanosine monophosphate content by neprilysin or phosphodiesterase 9 inhibition, and myocardial fibrosis by spironolactone. Because of phenotypic diversity in HFpEF, personalized therapeutic strategies are proposed, which are configured in a matrix with HFpEF presentations in the abscissa and HFpEF predispositions in the ordinate.
Keywords: diastole; heart failure; heart failure, diastolic; phenotype; therapeutics; ventricular function, left.
© 2016 American Heart Association, Inc.
Figures
References
-
- Borlaug BA. Heart Failure with Preserved Ejection Fraction. In: Baliga Ragavendra R., Haas Garrie J., editors. Management of Heart Failure. Springer Verlag; 2015.
-
- Paulus WJ, van Ballegoij JJ. Treatment of heart failure with normal ejection fraction: an inconvenient truth! J Am Coll Cardiol. 2010;55:526–37. - PubMed
-
- Holland DJ, Kumbhani DJ, Ahmed SH, Marwick TH. Effects of treatment on exercise tolerance, cardiac function, and mortality in heart failure with preserved ejection fraction. A meta-analysis. J Am Coll Cardiol. 2011;57:1676–86. - PubMed
-
- Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJV, Michelson EL, Olofsson B, Östergren J, for the CHARM Investigators and Committees Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362:777–781. - PubMed
-
- Anand IS, Rector TS, Cleland JG, Kuskowski M, McKelvie RS, Persson H, McMurray JJ, Zile MR, Komajda M, Massie BM, Carson PE. Prognostic value of baseline plasma amino-terminal pro-brain natriuretic peptide and its interactions with irbesartan treatment effects in patients with heart failure and preserved ejection fraction: findings from the I-PRESERVE trial. Circ Heart Fail. 2011;4:569–577. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
