

Combination Therapy with Anti-PD-1, Anti-TIM-3, and Focal Radiation Results in Regression of Murine Gliomas
- PMID: 27358487
- PMCID: PMC5735836
- DOI: 10.1158/1078-0432.CCR-15-1535
Combination Therapy with Anti-PD-1, Anti-TIM-3, and Focal Radiation Results in Regression of Murine Gliomas
Abstract
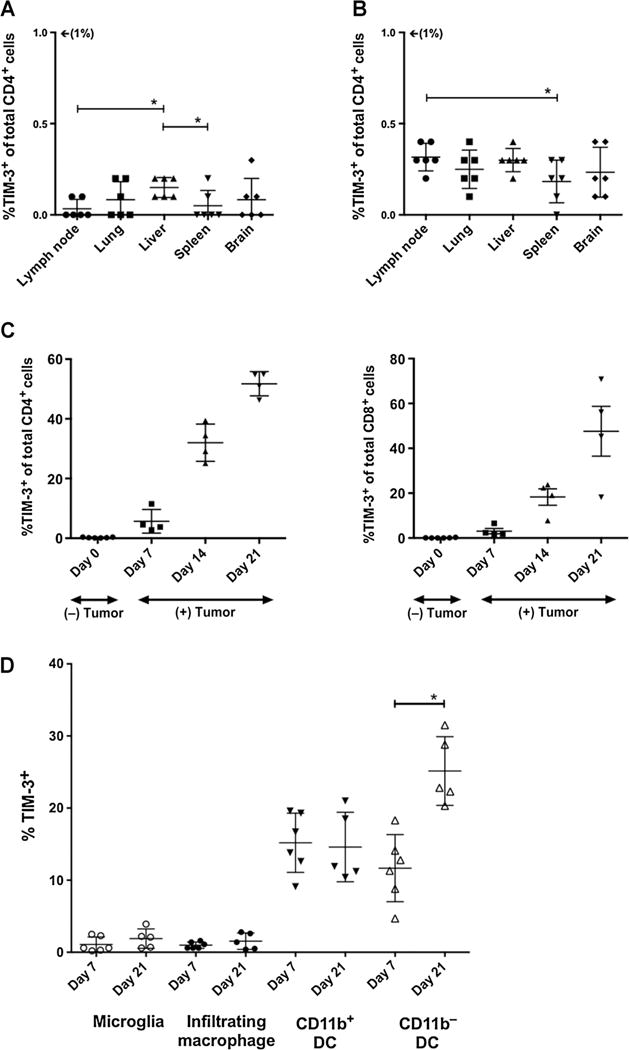
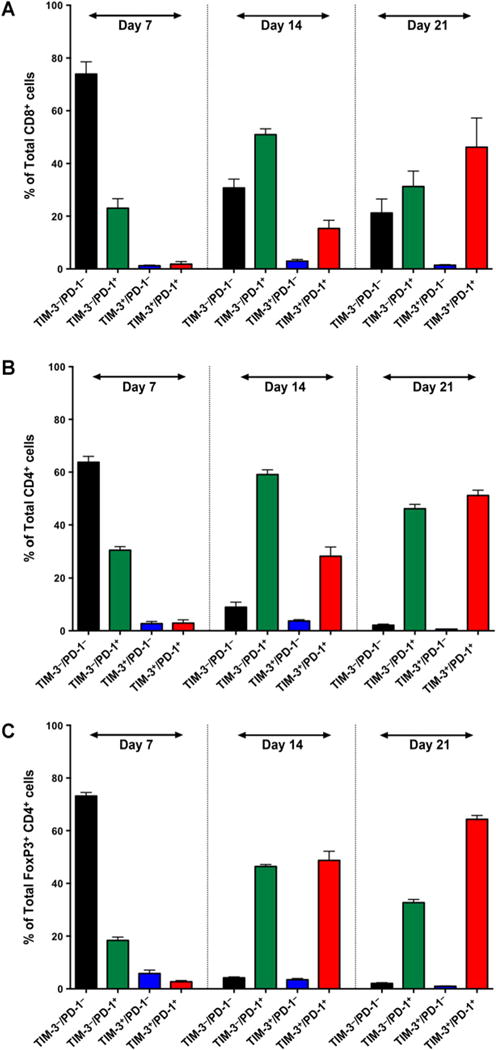
Purpose: Checkpoint molecules like programmed death-1 (PD-1) and T-cell immunoglobulin mucin-3 (TIM-3) are negative immune regulators that may be upregulated in the setting of glioblastoma multiforme. Combined PD-1 blockade and stereotactic radiosurgery (SRS) have been shown to improve antitumor immunity and produce long-term survivors in a murine glioma model. However, tumor-infiltrating lymphocytes (TIL) can express multiple checkpoints, and expression of ≥2 checkpoints corresponds to a more exhausted T-cell phenotype. We investigate TIM-3 expression in a glioma model and the antitumor efficacy of TIM-3 blockade alone and in combination with anti-PD-1 and SRS.
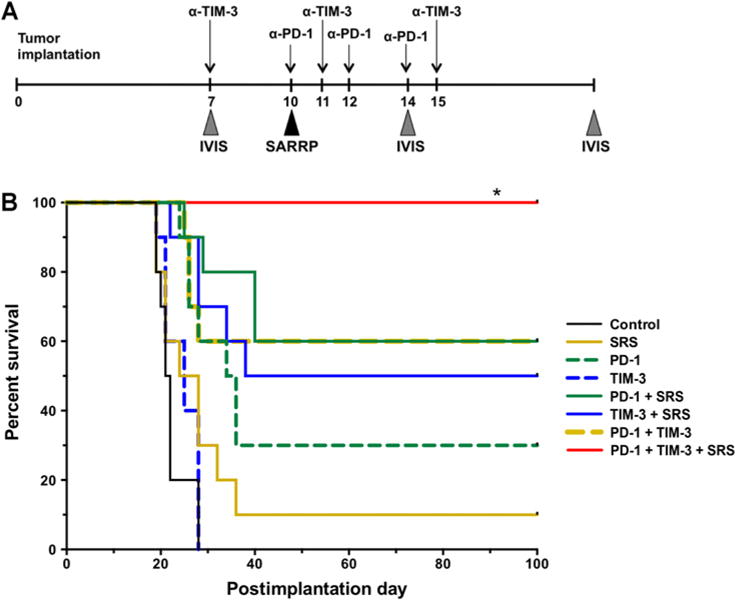
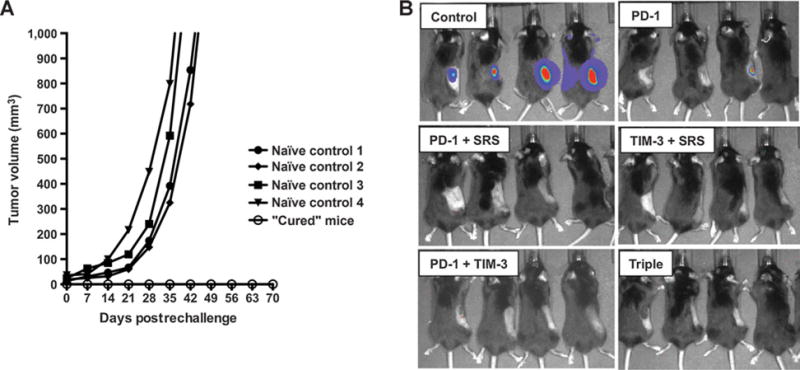
Experimental design: C57BL/6 mice were implanted with murine glioma cell line GL261-luc2 and randomized into 8 treatment arms: (i) control, (ii) SRS, (iii) anti-PD-1 antibody, (iv) anti-TIM-3 antibody, (v) anti-PD-1 + SRS, (vi) anti-TIM-3 + SRS, (vii) anti-PD-1 + anti-TIM-3, and (viii) anti-PD-1 + anti-TIM-3 + SRS. Survival and immune activation were assessed.
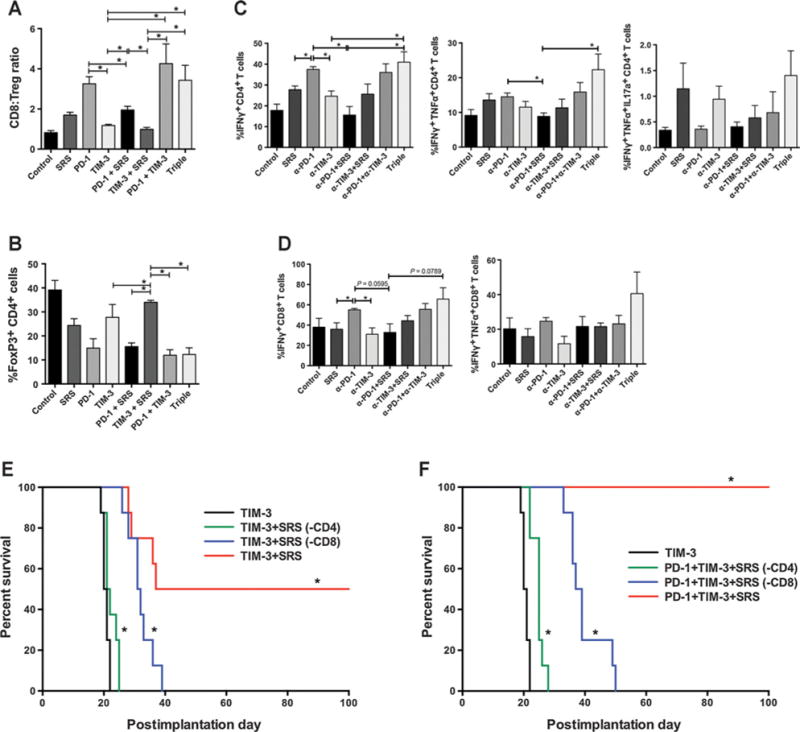
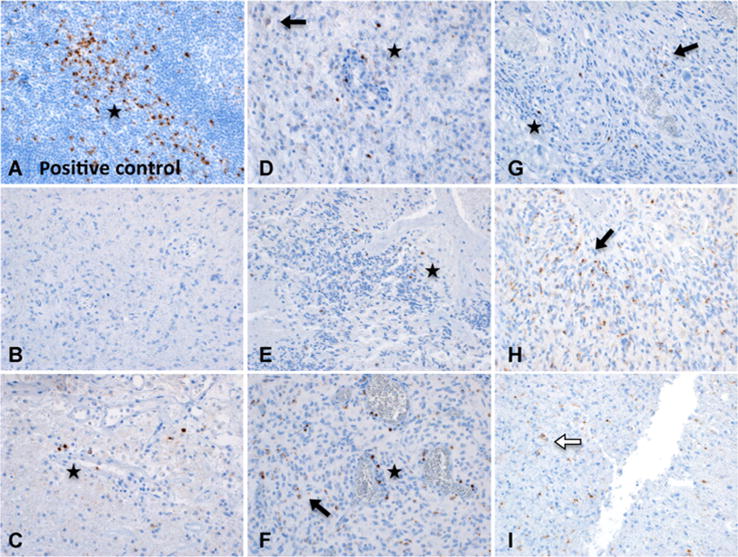
Results: Dual therapy with anti-TIM-3 antibody + SRS or anti-TIM-3 + anti-PD-1 improved survival compared with anti-TIM-3 antibody alone. Triple therapy resulted in 100% overall survival (P < 0.05), a significant improvement compared with other arms. Long-term survivors demonstrated increased immune cell infiltration and activity and immune memory. Finally, positive staining for TIM-3 was detected in 7 of 8 human GBM samples.
Conclusions: This is the first preclinical investigation on the effects of dual PD-1 and TIM-3 blockade with radiation. We also demonstrate the presence of TIM-3 in human glioblastoma multiforme and provide preclinical evidence for a novel treatment combination that can potentially result in long-term glioma survival and constitutes a novel immunotherapeutic strategy for the treatment of glioblastoma multiforme. Clin Cancer Res; 23(1); 124-36. ©2016 AACR.
©2016 American Association for Cancer Research.
Conflict of interest statement
No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–66. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
