

Prevalence, types and factors associated with echocardiographic abnormalities among newly diagnosed diabetic patients at Mulago Hospital
- PMID: 27358631
- PMCID: PMC4915408
- DOI: 10.4314/ahs.v16i1.25
Prevalence, types and factors associated with echocardiographic abnormalities among newly diagnosed diabetic patients at Mulago Hospital
Abstract
Background: The prevalence of Diabetes mellitus (DM) is on a rise in sub-Saharan Africa and will more than double by 2025. Cardiovascular disease (CVD) accounts for up to 2/3 of all deaths in the diabetic population. Of all the CVD deaths in DM, 3/4 occur in sub Saharan Africa (SSA). Non invasive identification of cardiac abnormalities, such as Left Ventricular Hypertrophy (LVH), diastolic and systolic dysfunction, is not part of diabetes complications surveillance programs in Uganda and there is limited data on this problem. This study sought to determine the prevalence, types and factors associated with echocardiographic abnormalities among newly diagnosed diabetic patients at Mulago National referral hospital in Uganda.
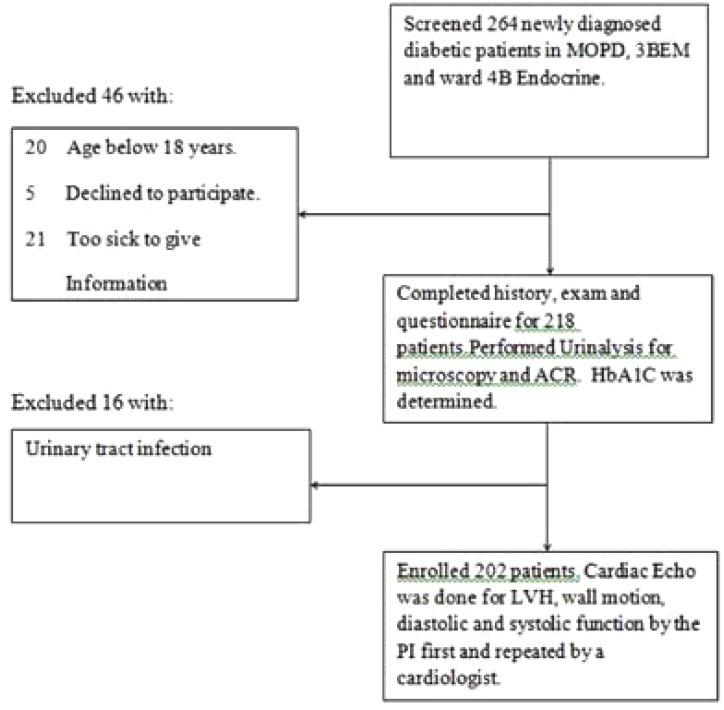
Methods: In this cross sectional study conducted between June 2014 and December 2014, we recruited 202 newly diagnosed adult diabetic patients. Information on patients' socio-demographics, bio-physical profile, biochemical testing and echocardiographic findings was obtained for all the participants using a pre-tested questionnaire. An abnormal echocardiogram in this study was defined as the presence of LVH, diastolic and/or systolic dysfunction and wall motion abnormality. Bivariate and multivariate logistic regression analyses were used to investigate the association of several parameters with echocardiographic abnormalities.
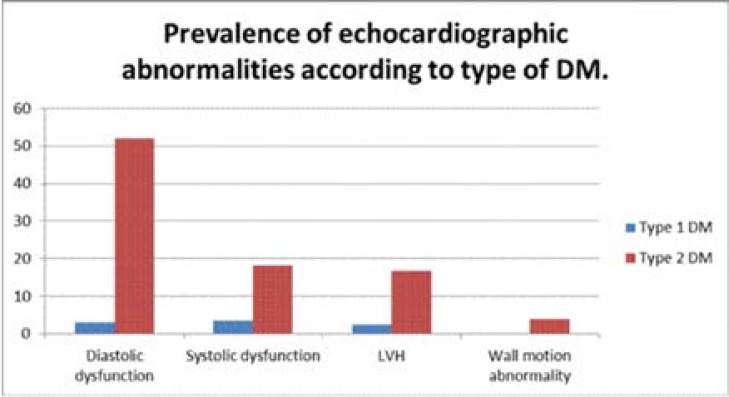
Results: Of the 202 patients recruited, males were 102(50.5%) and the mean age was 46±15 years. Majority of patients had type 2 DM, 156(77.2%) and type 1 DM, 41(20.3%) with mean HbA1C of 13.9±5.3%. Mean duration of diabetes was 2 months. The prevalence of an abnormal echocardiogram was 67.8 % (95% CI 60%-74%). Diastolic dysfunction, systolic dysfunction, LVH and wall motion abnormalities were present in 55.0%, 21.8%, 19.3% and 4.0% of all the participants respectively. In bivariate logistic regression analysis, the factors associated with an abnormal echocardiogram were age (OR 1.09 [95% CI 1.06-1.12], P <0.0001), type 2 DM (OR 5.8[95% CI 2.77-12.07], P<0.0001), hypertension (OR 2.64[95% CI 1.44-4.85], P=0.002), obesity (OR 3.51[955 CI 1.25-9.84], P=0.017 and increased waist circumference (OR 1.02[95% CI 1.00-1.04], P=0.024. On Multiple logistic regression analysis, age was the only factor associated with an abnormal echocardiogram (OR 1.09[95%CI 1.05-1.15], P<0.0001).
Conclusion: Echocardiographic abnormalities were common among newly diagnosed adults with DM. Traditional CVD risk factors were associated with an abnormal echocardiogram in this patient population. Due to a high prevalence of echocardiographic abnormalities among newly diagnosed diabetics, we recommend screening for cardiac disease especially in patients who present with traditional CVD risk factors. This will facilitate early diagnosis, management and hence better patient outcomes.
Keywords: Diabetes mellitus; cardiac abnormalities; echocardiography.
Figures
Similar articles
-
Hypertension among newly diagnosed diabetic patients at Mulago National Referral Hospital in Uganda: a cross sectional study.Cardiovasc J Afr. 2018 Jul/Aug 23;29(4):218-224. doi: 10.5830/CVJA-2018-015. Epub 2018 Apr 20. Cardiovasc J Afr. 2018. PMID: 29750228 Free PMC article.
-
Utility of albumin to creatinine ratio in screening for microalbuminuria among newly diagnosed diabetic patients in Uganda: a cross sectional study.Afr Health Sci. 2019 Mar;19(1):1607-1616. doi: 10.4314/ahs.v19i1.36. Afr Health Sci. 2019. PMID: 31148990 Free PMC article.
-
Microalbuminuria and left ventricular hypertrophy among newly diagnosed black African hypertensive patients: a cross sectional study from a tertiary hospital in Uganda.BMC Res Notes. 2015 May 14;8:198. doi: 10.1186/s13104-015-1156-2. BMC Res Notes. 2015. PMID: 25971452 Free PMC article.
-
The prevalence of left ventricular diastolic dysfunction and heart failure with preserved ejection fraction in men and women with type 2 diabetes: A systematic review and meta-analysis.Diab Vasc Dis Res. 2018 Nov;15(6):477-493. doi: 10.1177/1479164118787415. Epub 2018 Jul 24. Diab Vasc Dis Res. 2018. PMID: 30037278 Free PMC article.
-
Prevalence rate of left ventricular hypertrophy and the burden of arrhythmias among hypertensive patients attending Jinja Regional Referral Hospital, eastern Uganda.Curr Probl Cardiol. 2024 Sep;49(9):102741. doi: 10.1016/j.cpcardiol.2024.102741. Epub 2024 Jul 6. Curr Probl Cardiol. 2024. PMID: 38972469 Review.
Cited by
-
Association of body mass index with left ventricular diastolic dysfunction among ambulatory individuals with diabetes mellitus in rural Uganda: a cross-sectional study.BMC Cardiovasc Disord. 2022 Jun 20;22(1):279. doi: 10.1186/s12872-022-02718-2. BMC Cardiovasc Disord. 2022. PMID: 35725371 Free PMC article.
-
Microalbuminuria and Traditional Serum Biomarkers of Nephropathy among Diabetic Patients at Mbarara Regional Referral Hospital in South Western Uganda.J Diabetes Res. 2019 Dec 16;2019:3534260. doi: 10.1155/2019/3534260. eCollection 2019. J Diabetes Res. 2019. PMID: 31934589 Free PMC article.
-
Assessment of electrocardiogram abnormality and associated factors among apparently healthy adult type 2 diabetic patients on follow-up at Jimma Medical Center, Southwest Ethiopia: Cross-sectional study.BMC Cardiovasc Disord. 2021 Jun 24;21(1):312. doi: 10.1186/s12872-021-02110-6. BMC Cardiovasc Disord. 2021. PMID: 34167465 Free PMC article.
-
Indicators of optimal diabetes care and burden of diabetes complications in Africa: a systematic review and meta-analysis.BMJ Open. 2022 Nov 8;12(11):e060786. doi: 10.1136/bmjopen-2022-060786. BMJ Open. 2022. PMID: 36351737 Free PMC article.
-
A study of electrocardiographic and 2D echocardiographic changes in type 2 diabetes mellitus patients without cardiovascular symptoms.J Family Med Prim Care. 2022 Mar;11(3):1036-1039. doi: 10.4103/jfmpc.jfmpc_1195_21. Epub 2022 Mar 10. J Family Med Prim Care. 2022. PMID: 35495842 Free PMC article.
References
-
- Goodarz D, Carlene M, Lawes, Stephen V, Hoorn, Christopher J, et al. Global and regional mortality from ischaemic heart disease and stroke attributable to higher-than-optimum blood glucose concentration: comparative risk assessment. Lancet. 2006;368:1651–1659. - PubMed
-
- Amos A, McCarty D. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet Med. 1997;14(suppl 5):S1–S85. - PubMed
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. - PubMed
-
- André PK, Albert GB, Amoah, Mbanya Jean-Claude. Cardiovascular Complications of Diabetes Mellitus in Sub-Saharan Africa. Circulation. 2005;112:3592–3601. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials