

Targeted Temperature Management After Pediatric Cardiac Arrest Due To Drowning: Outcomes and Complications
- PMID: 27362855
- PMCID: PMC5123789
- DOI: 10.1097/PCC.0000000000000763
Targeted Temperature Management After Pediatric Cardiac Arrest Due To Drowning: Outcomes and Complications
Abstract
Objective: To describe outcomes and complications in the drowning subgroup from the Therapeutic Hypothermia After Pediatric Cardiac Arrest Out-of-Hospital trial.
Design: Exploratory post hoc cohort analysis.
Setting: Twenty-four PICUs.
Patients: Pediatric drowning cases.
Interventions: Therapeutic hypothermia versus therapeutic normothermia.
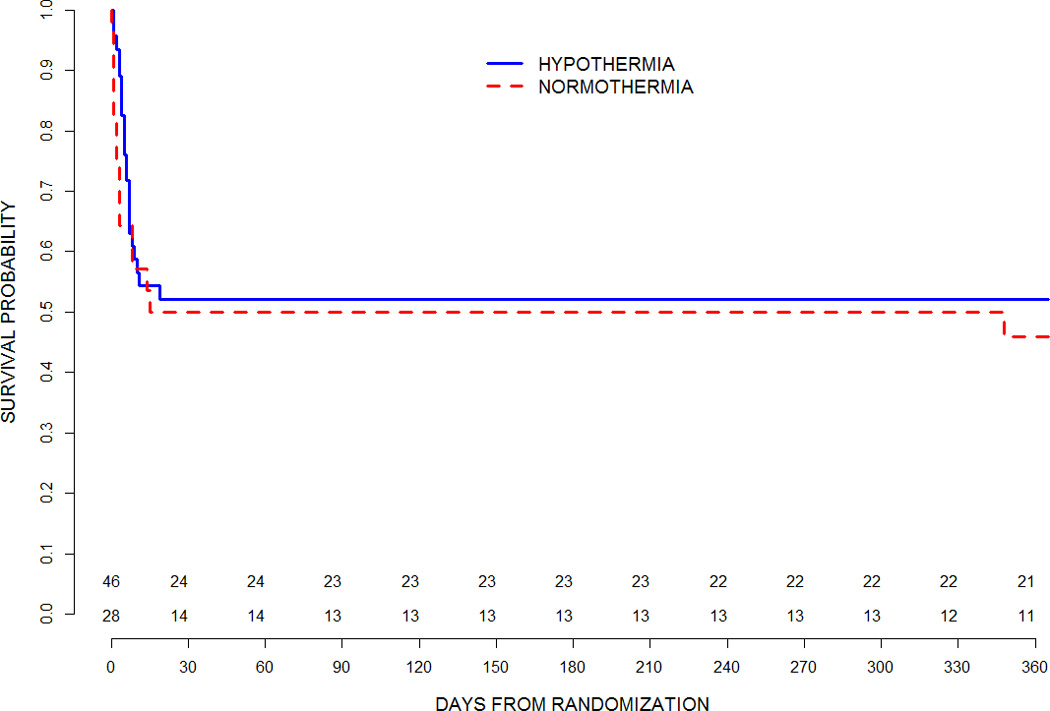
Measurements and main results: An exploratory study of pediatric drowning from the Therapeutic Hypothermia After Pediatric Cardiac Arrest Out-of-Hospital trial was conducted. Comatose patients aged more than 2 days and less than 18 years were randomized up to 6 hours following return-of-circulation to hypothermia (n = 46) or normothermia (n = 28). Outcomes assessed included 12-month survival with a Vineland Adaptive Behavior Scale score of greater than or equal to 70, 1-year survival rate, change in Vineland Adaptive Behavior Scale-II score from prearrest to 12 months, and select safety measures. Seventy-four drowning cases were randomized. In patients with prearrest Vineland Adaptive Behavior Scale-II greater than or equal to 70 (n = 65), there was no difference in 12-month survival with Vineland Adaptive Behavior Scale-II score of greater than or equal to 70 between hypothermia and normothermia groups (29% vs 17%; relative risk, 1.74; 95% CI, 0.61-4.95; p = 0.27). Among all evaluable patients (n = 68), the Vineland Adaptive Behavior Scale-II score change from baseline to 12 months did not differ (p = 0.46), and 1-year survival was similar (49% hypothermia vs 42%, normothermia; relative risk, 1.16; 95% CI, 0.68-1.99; p = 0.58). Hypothermia was associated with a higher prevalence of positive bacterial culture (any blood, urine, or respiratory sample; 67% vs 43%; p = 0.04); however, the rate per 100 days at risk did not differ (11.1 vs 8.4; p = 0.46). Cumulative incidence of blood product use, serious arrhythmias, and 28-day mortality were not different. Among patients with cardiopulmonary resuscitation durations more than 30 minutes or epinephrine doses greater than 4, none had favorable Pediatric Cerebral Performance Category outcomes (≤ 3).
Conclusions: In comatose survivors of out-of-hospital pediatric cardiac arrest due to drowning, hypothermia did not result in a statistically significant benefit in survival with good functional outcome or mortality at 1 year, as compared with normothermia. High risk of culture-proven bacterial infection was observed in both groups.
Figures
Comment in
-
Targeted Temperature Management After Cardiac Arrest Due to Drowning: "Frequentist" and "Bayesian" Decision Making.Pediatr Crit Care Med. 2016 Aug;17(8):789-91. doi: 10.1097/PCC.0000000000000799. Pediatr Crit Care Med. 2016. PMID: 27500613 Free PMC article. No abstract available.
References
-
- Young KD, Gausche-Hill M, McClung CD, Lewis RJ. A prospective, population-based study of the epidemiology and outcome of out-of-hospital pediatric cardiopulmonary arrest. Pediatrics. 2004;114:157–164. - PubMed
-
- Donoghue AJ, Nadkarni V, Berg RA, et al. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge. Ann Emerg Med. 2005;46:512–522. - PubMed
-
- Mild therapeutic hypothermia to improve the neurological outcome after cardiac arrest. The Hypothermia After Cardiac Arrest Study Group. N Engl J Med. 2002;346:549–556. - PubMed
-
- Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557–563. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- R21 HD044955/HD/NICHD NIH HHS/United States
- U54 HD079123/HD/NICHD NIH HHS/United States
- R34 HD050531/HD/NICHD NIH HHS/United States
- UL1 TR001878/TR/NCATS NIH HHS/United States
- U10 HD049945/HD/NICHD NIH HHS/United States
- P30 HD040677/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UL1 RR024986/RR/NCRR NIH HHS/United States
- U01 HL094339/HL/NHLBI NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- U01 HL094345/HL/NHLBI NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
