

Field Assessment Stroke Triage for Emergency Destination: A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes
- PMID: 27364531
- PMCID: PMC4961538
- DOI: 10.1161/STROKEAHA.116.013301
Field Assessment Stroke Triage for Emergency Destination: A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes
Abstract
Background and purpose: Patients with large vessel occlusion strokes (LVOS) may be better served by direct transfer to endovascular capable centers avoiding hazardous delays between primary and comprehensive stroke centers. However, accurate stroke field triage remains challenging. We aimed to develop a simple field scale to identify LVOS.
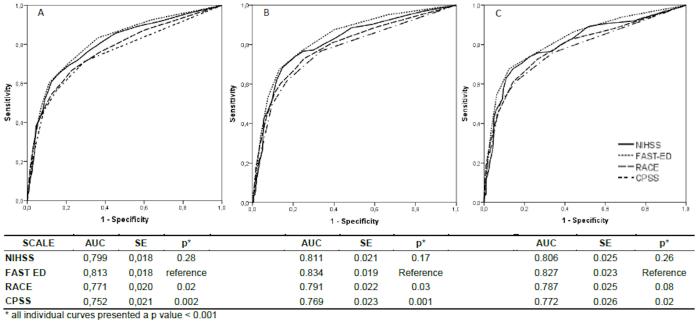
Methods: The Field Assessment Stroke Triage for Emergency Destination (FAST-ED) scale was based on items of the National Institutes of Health Stroke Scale (NIHSS) with higher predictive value for LVOS and tested in the Screening Technology and Outcomes Project in Stroke (STOPStroke) cohort, in which patients underwent computed tomographic angiography within the first 24 hours of stroke onset. LVOS were defined by total occlusions involving the intracranial internal carotid artery, middle cerebral artery-M1, middle cerebral artery-2, or basilar arteries. Patients with partial, bihemispheric, and anterior+posterior circulation occlusions were excluded. Receiver operating characteristic curve, sensitivity, specificity, positive predictive value, and negative predictive value of FAST-ED were compared with the NIHSS, Rapid Arterial Occlusion Evaluation (RACE) scale, and Cincinnati Prehospital Stroke Severity (CPSS) scale.
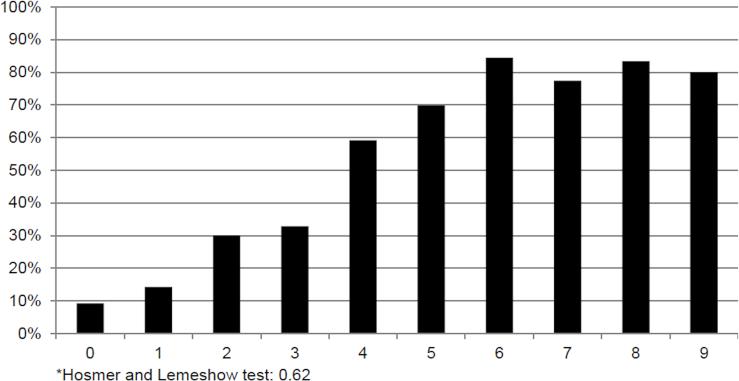
Results: LVO was detected in 240 of the 727 qualifying patients (33%). FAST-ED had comparable accuracy to predict LVO to the NIHSS and higher accuracy than RACE and CPSS (area under the receiver operating characteristic curve: FAST-ED=0.81 as reference; NIHSS=0.80, P=0.28; RACE=0.77, P=0.02; and CPSS=0.75, P=0.002). A FAST-ED ≥4 had sensitivity of 0.60, specificity of 0.89, positive predictive value of 0.72, and negative predictive value of 0.82 versus RACE ≥5 of 0.55, 0.87, 0.68, and 0.79, and CPSS ≥2 of 0.56, 0.85, 0.65, and 0.78, respectively.
Conclusions: FAST-ED is a simple scale that if successfully validated in the field, it may be used by medical emergency professionals to identify LVOS in the prehospital setting enabling rapid triage of patients.
Keywords: cerebrovascular occlusion; scale; stroke, acute, prehospital emergency care; triage.
© 2016 American Heart Association, Inc.
Figures
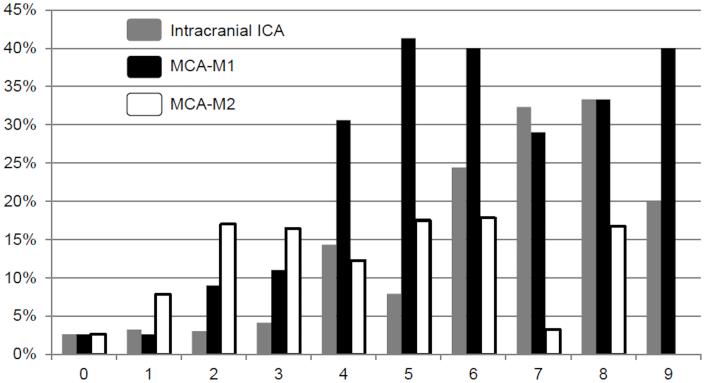
 Intracranial ICA
Intracranial ICA  MCA-M1
MCA-M1  MCA-M2
MCA-M2Comment in
-
Letter by Heldner et al Regarding Article, "Field Assessment Stroke Triage for Emergency Destination: A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes".Stroke. 2016 Dec;47(12):e274. doi: 10.1161/STROKEAHA.116.015219. Epub 2016 Nov 10. Stroke. 2016. PMID: 27834747 No abstract available.
-
Response by Lima et al to Letter Regarding Article, "Field Assessment Stroke Triage for Emergency Destination: A Simple and Accurate Prehospital Scale to Detect Large Vessel Occlusion Strokes".Stroke. 2016 Dec;47(12):e275-e276. doi: 10.1161/STROKEAHA.116.015296. Epub 2016 Nov 10. Stroke. 2016. PMID: 27834749 Free PMC article. No abstract available.
References
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. - PubMed
-
- Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. Stent-retriever thrombectomy after intravenous t-pa vs. T-pa alone in stroke. N Engl J Med. 2015;372:2285–2295. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–1018. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372:1019–1030. - PubMed
-
- Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372:2296–2306. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
