

Acute Rejection Rates and Graft Outcomes According to Induction Regimen among Recipients of Kidneys from Deceased Donors Treated with Tacrolimus and Mycophenolate
- PMID: 27364616
- PMCID: PMC5012491
- DOI: 10.2215/CJN.13171215
Acute Rejection Rates and Graft Outcomes According to Induction Regimen among Recipients of Kidneys from Deceased Donors Treated with Tacrolimus and Mycophenolate
Abstract
Background and objectives: IL-2 receptor antagonist (IL2-RA) is recommended as a first-line agent for induction therapy in renal transplantation. However, this remains controversial in deceased donor renal transplantation (DDRT) maintained on tacrolimus (TAC)/mycophenolic acid (MPA) with or without steroids.
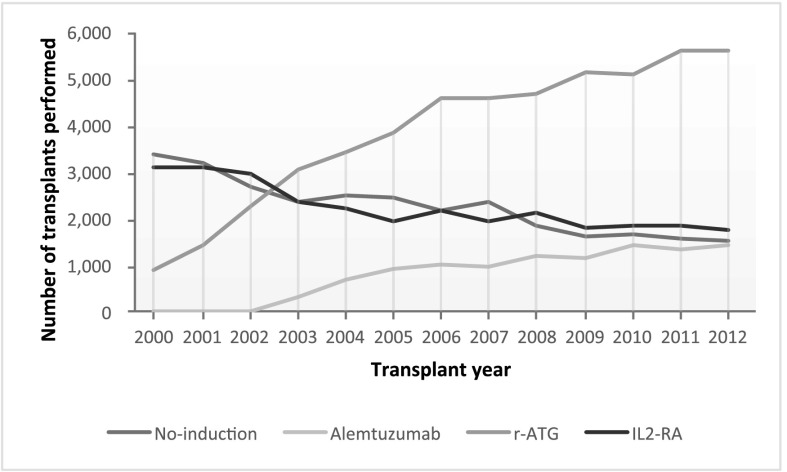
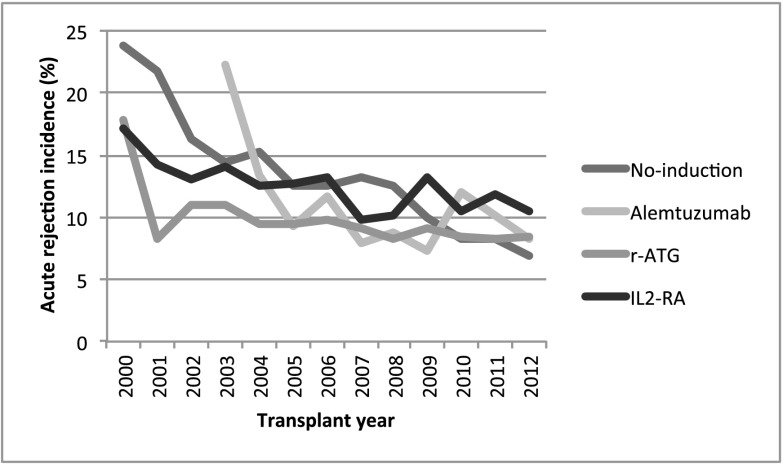
Design, setting, participants, & measurements: We studied the United Network for Organ Sharing Registry for patients receiving DDRT from 2000 to 2012 maintained on TAC/MPA at transplantation hospital discharge (n=74,627) to compare outcomes of IL2-RA and other induction agents. We initially divided the cohort into two groups on the basis of steroid use at the time of discharge: steroid (n=59,010) versus no steroid (n=15,617). Each group was stratified into induction categories: IL2-RA, rabbit antithymocyte globulin (r-ATG), alemtuzumab, and no induction. The main outcomes were incidence of acute rejection within the first year and overall graft failure (defined as graft failure and/or death) post-transplantation. Propensity score (PS), specifically inverse probability of treatment weight, analysis was used to minimize selection bias caused by nonrandom assignment of induction therapies.
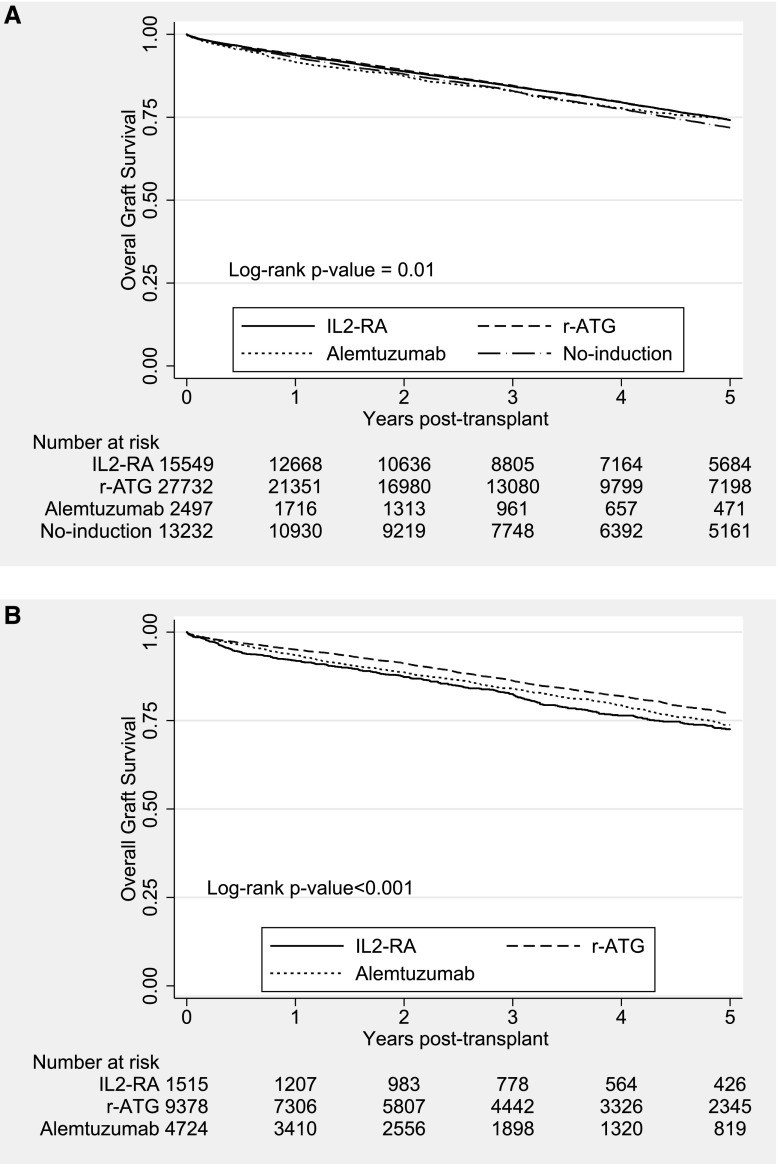
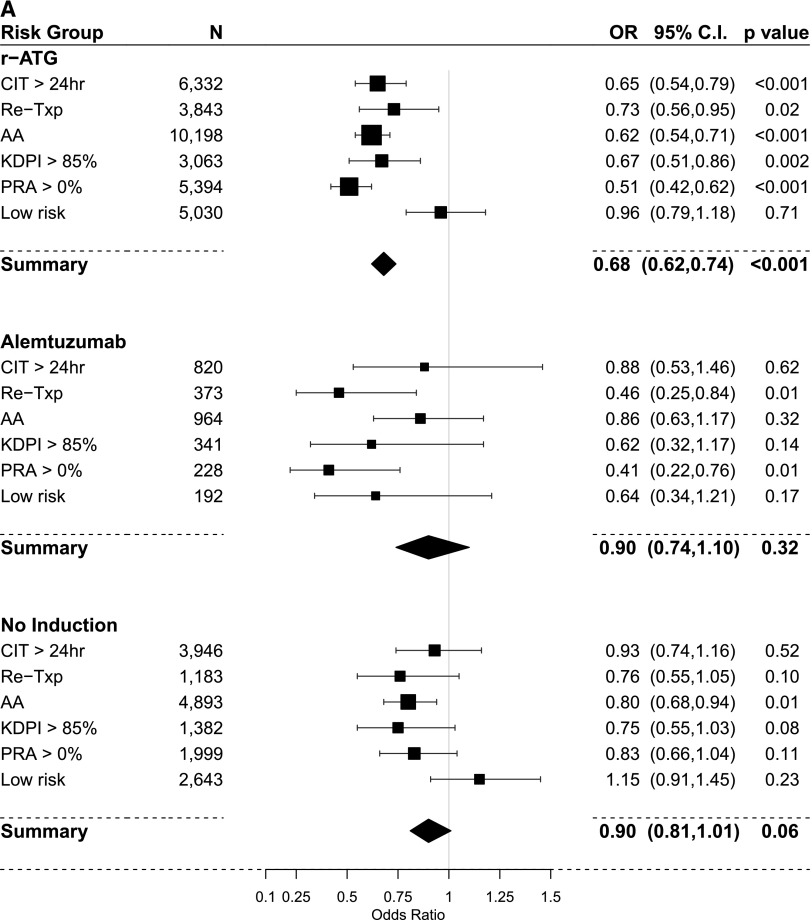
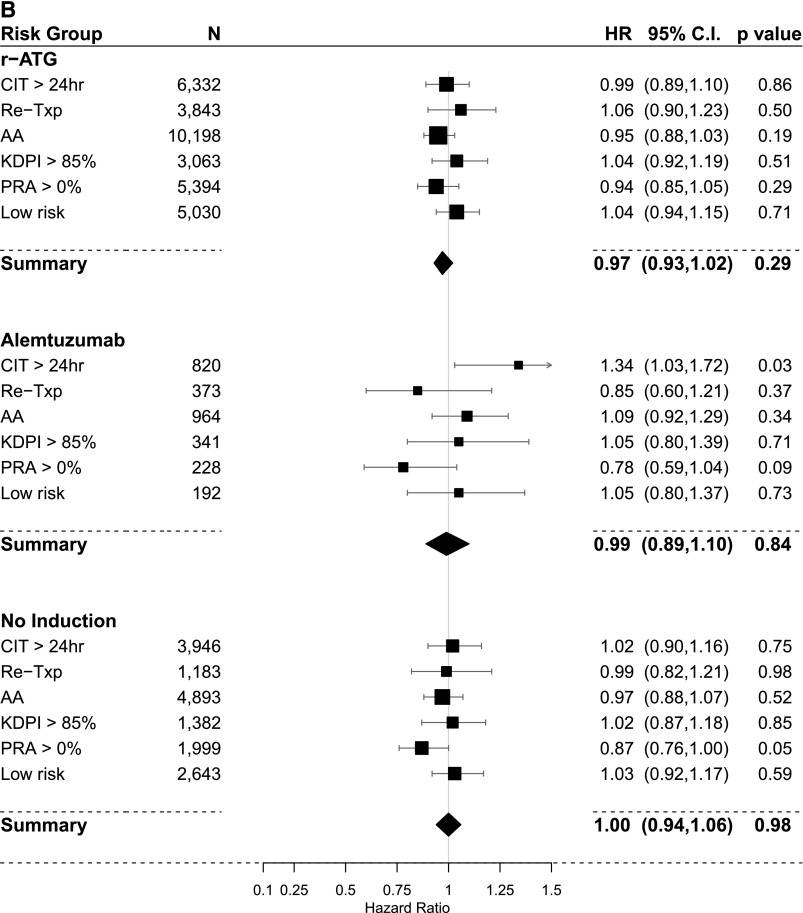
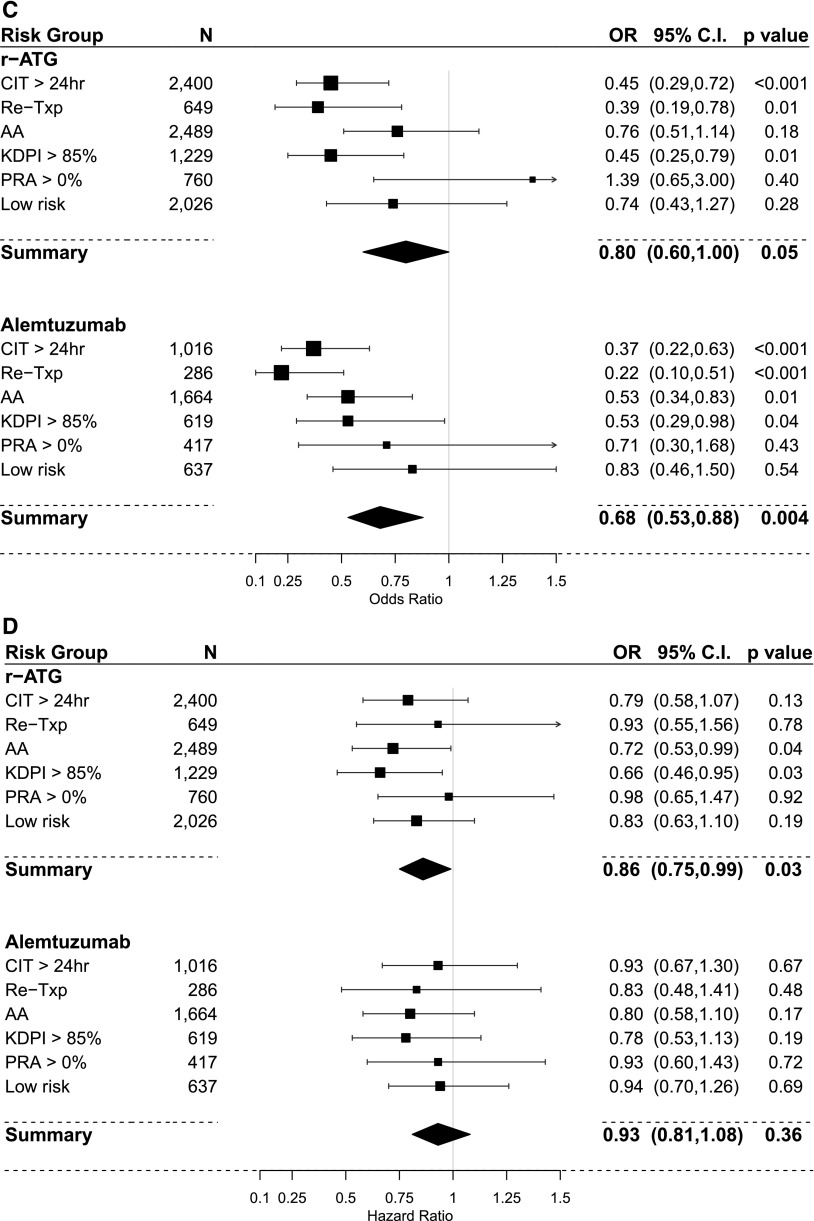
Results: Median (25th, 75th percentiles) follow-up times were 3.9 (1.1, 5.9) and 3.2 (1.1, 4.9) years for steroid and no steroid groups, respectively. Acute rejection within the first year and overall graft failure within 5 years of transplantation were more common in the no induction category (13.3%; P<0.001 and 28%; P=0.01, respectively) in the steroid group and the IL2-RA category (11.1%; P=0.16 and 27.4%; P<0.001, respectively) in the no steroid group. Compared with IL2-RA, PS-weighted and covariate-adjusted multivariable logistic and Cox analyses showed that outcomes in the steroid group were similar among induction categories, except that acute rejection was significantly lower with r-ATG (odds ratio [OR], 0.68; 95% confidence interval [95% CI], 0.62 to 0.74). In the no steroid group, compared with IL2-RA, odds of acute rejection with r-ATG (OR, 0.80; 95% CI, 0.60 to 1.00) and alemtuzumab (OR, 0.68; 95% CI, 0.53 to 0.88) were lower, and r-ATG was associated with better graft survival (hazard ratio, 0.86; 95% CI, 0.75 to 0.99).
Conclusions: In DDRT, compared with IL2-RA induction, no induction was associated with similar outcomes when TAC/MPA/steroids were used. r-ATG seems to offer better graft survival over IL2-RA in steroid avoidance protocols.
Keywords: Antibodies, Monoclonal, Humanized; Antilymphocyte Serum; Follow-Up Studies; Graft Survival; Humans; Immunosuppression; Immunosuppressive Agents; Mycophenolic Acid; Tissue Donors; kidney transplantation; rejection; tacrolimus.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Hardinger KL, Brennan DC, Klein CL: Selection of induction therapy in kidney transplantation. Transpl Int 26: 662–672, 2013 - PubMed
-
- Matas AJ, Smith JM, Skeans MA, Thompson B, Gustafson SK, Schnitzler MA, Stewart DE, Cherikh WS, Wainright JL, Snyder JJ, Israni AK, Kasiske BL: OPTN/SRTR 2012 Annual Data Report: Kidney. Am J Transplant 14[Suppl 1]: 11–44, 2014 - PubMed
-
- Bia M, Adey DB, Bloom RD, Chan L, Kulkarni S, Tomlanovich S: KDOQI US commentary on the 2009 KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Kidney Dis 56: 189–218, 2010 - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group: KDIGO clinical practice guideline for the care of kidney transplant recipients. Am J Transplant 9[Suppl 3]: S1–S155, 2009 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
