

The Severity of Bleeding and Mortality in Trauma Patients Taking Dabigatran
- PMID: 27364823
- PMCID: PMC5482216
- DOI: 10.1016/j.jemermed.2016.05.005
The Severity of Bleeding and Mortality in Trauma Patients Taking Dabigatran
Abstract
Background: Dabigatran, a direct thrombin inhibitor, has been shown to be more effective than warfarin in the prevention of stroke in patients with atrial fibrillation. Until recently, it lacked a reversal agent, and its contribution to the risk of transfusion in injured patients is unknown.
Objective: We sought to determine whether patients who sustain traumatic injuries while taking dabigatran receive more blood transfusions than matched patients taking warfarin, aspirin, clopidogrel, or controls.
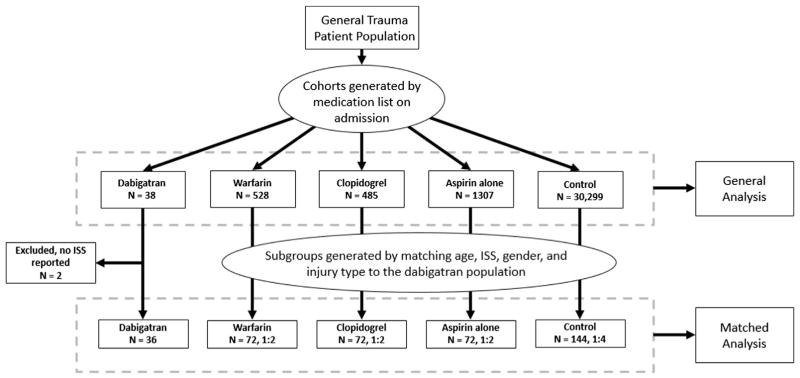
Methods: This retrospective, single-center cohort consisted of injured patients who were taking dabigatran before admission to a major trauma center (January 2010-December 2013) who were compared with cohorts of patients taking warfarin, clopidogrel, or aspirin and a control group. The outcome was bleeding risk as measured by the use of blood products, with mortality as a secondary outcome. Outcomes were controlled for by age, sex, injury severity, and blunt mechanism.
Results: Thirty-eight patients were taking dabigatran. Compared with the general trauma population, patients taking dabigatran were more likely to be male, older, and to have higher injury severity. Patients taking dabigatran received transfusions (odds ratio [OR] 1.31 [95% confidence interval {CI} 0.56-3.04]), packed red blood cells (OR 1.43 [95% CI 0.54-3.77]), frozen plasma (OR 1.20 [95% CI 0.42-3.49]), and platelets (OR 2.01 [95% CI 0.63-6.37]) as often as matched controls. The mortality rate among patients on dabigatran was 12.5% (OR 1.51 [95% CI 0.39-5.89]) compared with 9.1% in matched controls. None of these results was statistically significant.
Conclusions: In this small study, injured patients taking dabigatran were transfused as often and had similar in-hospital mortality as matched controls who were not taking anticoagulants.
Keywords: dabigatran; epidemiology; hematology; mortality; transfusion; trauma.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Dabigatran: Important Considerations in the Elderly.J Emerg Med. 2017 Jun;52(6):884. doi: 10.1016/j.jemermed.2016.11.062. Epub 2017 Mar 23. J Emerg Med. 2017. PMID: 28343796 No abstract available.
References
-
- Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition) Chest. 2008;133(6 suppl):381S–453. - PubMed
-
- Goldhaber SZ, Fanikos J. Prevention of deep vein thrombosis and pulmonary embolism. Circulation. 2004;110:e445–7. - PubMed
-
- Kushner FG, Hand M, Smith SC, Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 Guildine and 2007 Focused Update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2009;120:2271–306. - PubMed
-
- Wann LS, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (update on dabigatran): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;123:1144–50. - PubMed
-
- Budnitz DS, Pollock DA, Weidenbach KN, et al. National Surveillance of emergency department visits for outpatient adverse drug events. JAMA. 2006;296:1858–66. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
