

Do serial measurements of cervical length improve the prediction of preterm birth in asymptomatic women with twin gestations?
- PMID: 27365003
- PMCID: PMC5086275
- DOI: 10.1016/j.ajog.2016.06.034
Do serial measurements of cervical length improve the prediction of preterm birth in asymptomatic women with twin gestations?
Abstract
Background: Cervical length at midtrimester is a powerful predictor of preterm birth in twin gestations. However, given the fact that, in some cases, cervical shortening may become evident only later during the second trimester, it seems reasonable that serial monitoring of cervical length may improve the detection of preterm birth in women with twins. However, data in support of such a practice are limited and conflicting. The contradictory results may be related to the fact that in most of these studies, the analysis of the predictive value of serial measurements of cervical length was limited to data derived from only two sequential measurements of cervical length, while data on the predictive value of multiple (>2) measurements are scarce.
Objective: We sought to determine whether serial measurements of cervical length can improve the prediction of preterm birth in asymptomatic women with twin gestations compared with a single measurement of cervical length at midgestation.
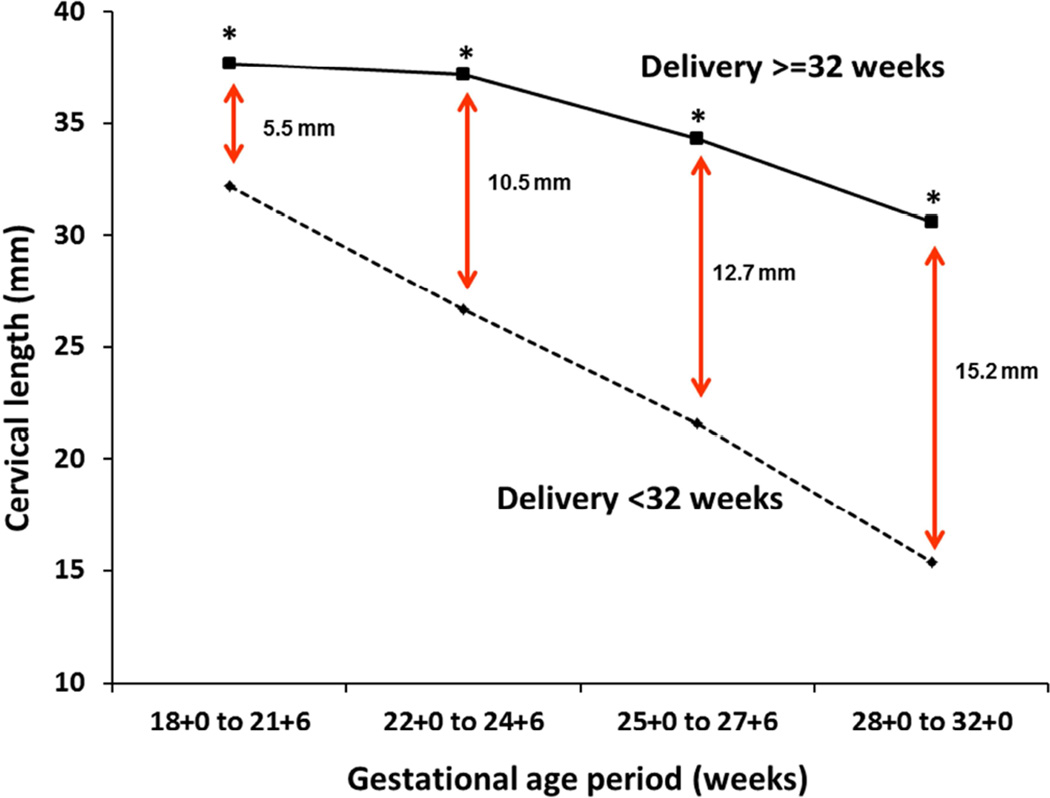
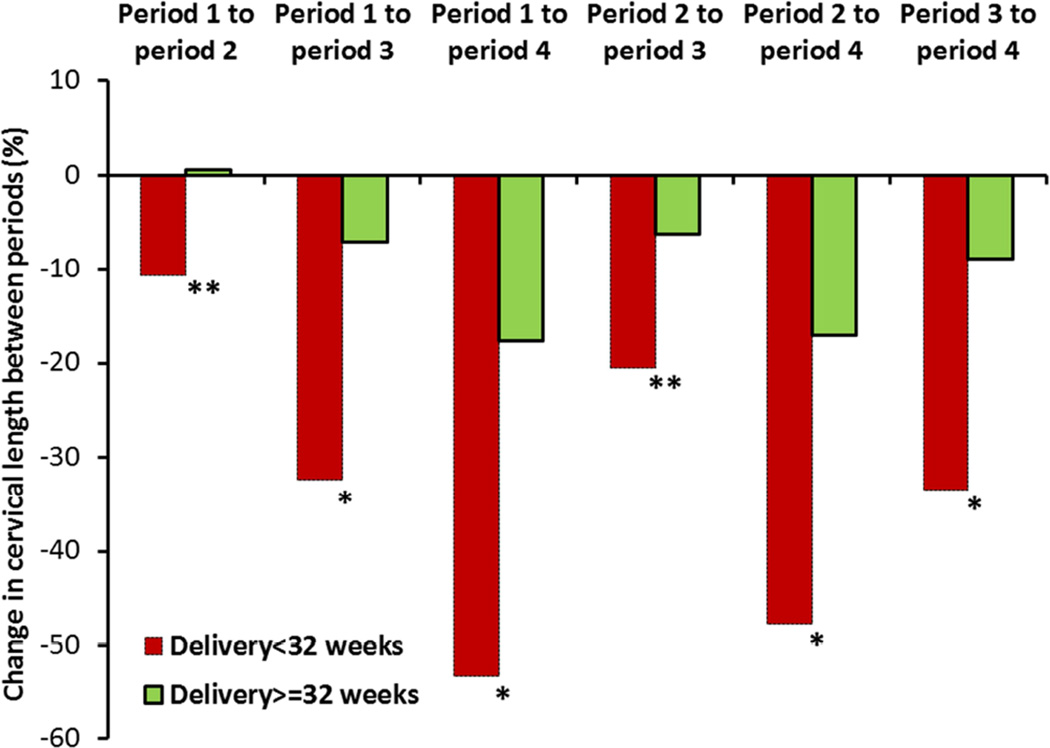
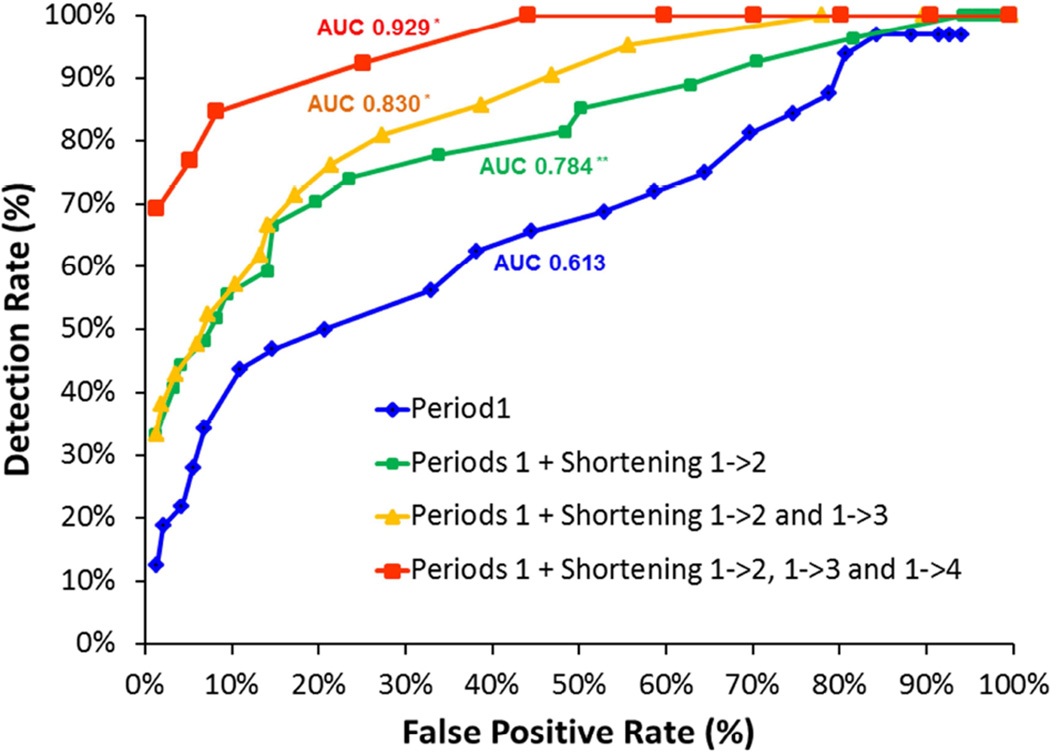
Study design: This was a retrospective cohort study of women with twin pregnancies followed up in a tertiary medical center from 2012 through 2014. All participants underwent routine measurement of cervical length at midgestation and every 2-3 weeks thereafter until 28-32 weeks. For each patient, cervical length was determined at the following time periods: 18+0 to 21+6 weeks (period 1, routine exam), 22+0 to 24+6 weeks (period 2), 25+0 to 27+6 weeks (period 3), and 28+0 to 32+0 weeks (period 4). Measurements of cervical length at periods 2-4 were analyzed in the form of either absolute length (in millimeters) or percent shortening relative to cervical length at period 1. The performance of a stepwise algorithm that incorporated serial measurements of cervical length for the prediction of preterm birth was compared to that achieved with a single measurement of cervical length at period 1.
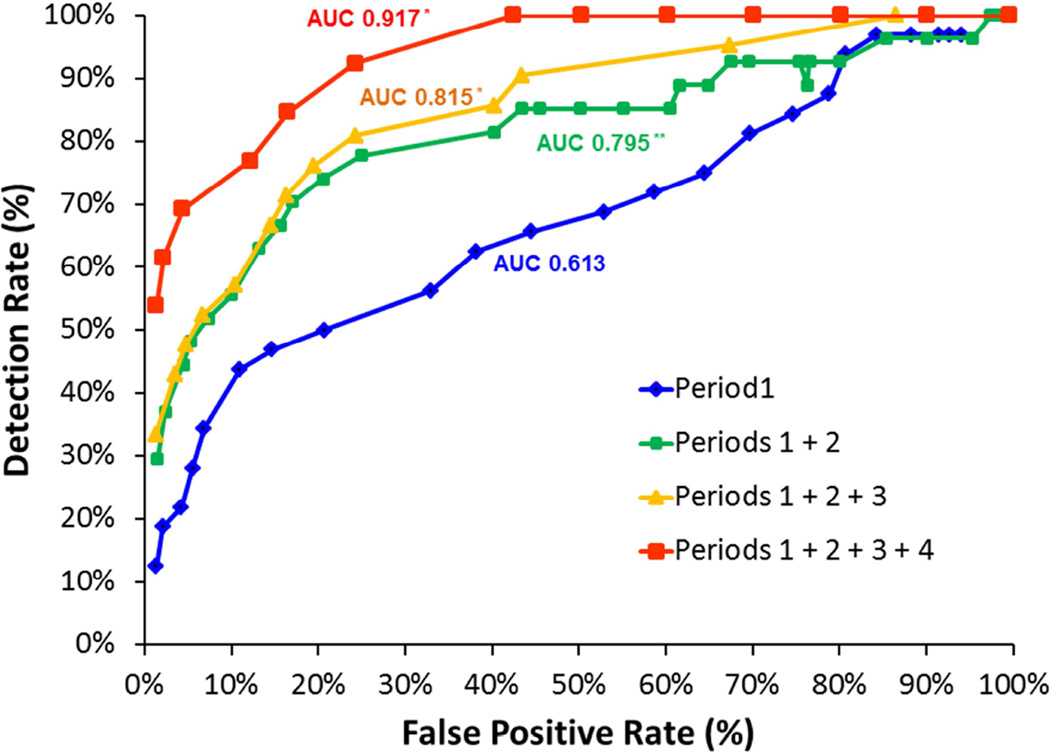
Results: Overall, 441 women with twin pregnancies who were eligible for the study underwent a total of 2374 cervical length measurements. The association of a short cervix (<10th percentile) with preterm birth at <32 weeks persisted in each of the 4 periods of gestation [odds ratio (95% confidence interval): 7.2 (3.1-16.5), 15.3 (6.4-36.7), 10.3 (4.4-24.3), and 23.1(8.3-64.1), respectively]. Compared with a single measurement of cervical length at midgestation (period 1), a stepwise algorithm integrating serial cervical length measurements from all 4 successive gestational age periods resulted in a significant increase in the area under the receiver operating characteristic curve (0.917 vs 0.613, P < .001). Similarly, when a target false-positive rate of 5% was used, the same stepwise algorithm was associated with a higher detection rate (69% vs 28%, P < .001), higher positive likelihood ratio (14.54 vs 5.12), and lower negative likelihood ratio (0.32 vs 0.76) for preterm birth at <32 weeks compared with a single measurement of cervical length at period 1.
Conclusion: Integration of serial measurements of cervical length using a stepwise algorithm in asymptomatic women with twin gestations can improve the detection of women at risk of preterm birth. Prospective studies are needed to validate these findings, and to investigate whether improved risk assessment performance is sufficient to offset the additional costs associated with serial cervical length measurements.
Keywords: biomarker; cervical ripening; cervical shortening; cervix; labor; longitudinal study; prediction; pregnancy; prematurity; preterm labor; screening; ultrasound.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
statement: The authors report no conflict of interest.
Figures
References
-
- Garite TJ, Clark RH, Elliott JP, Thorp JA. Twins and triplets: the effect of plurality and growth on neonatal outcome compared with singleton infants. American journal of obstetrics and gynecology. 2004;191:700–707. - PubMed
-
- Shinwell ES, Blickstein I. The risks for very low birth weight infants from multiple pregnancies. Clinics in perinatology. 2007;34:587–597. vi–vii. - PubMed
-
- Chauhan SP, Scardo JA, Hayes E, Abuhamad AZ, Berghella V. Twins: prevalence, problems, and preterm births. American journal of obstetrics and gynecology. 2010;203:305–315. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
