

Maximising HIV prevention by balancing the opportunities of today with the promises of tomorrow: a modelling study
- PMID: 27365203
- PMCID: PMC4935669
- DOI: 10.1016/S2352-3018(16)30036-4
Maximising HIV prevention by balancing the opportunities of today with the promises of tomorrow: a modelling study
Abstract
Background: Many ways of preventing HIV infection have been proposed and more are being developed. We sought to construct a strategic approach to HIV prevention that would use limited resources to achieve the greatest possible prevention impact through the use of interventions available today and in the coming years.
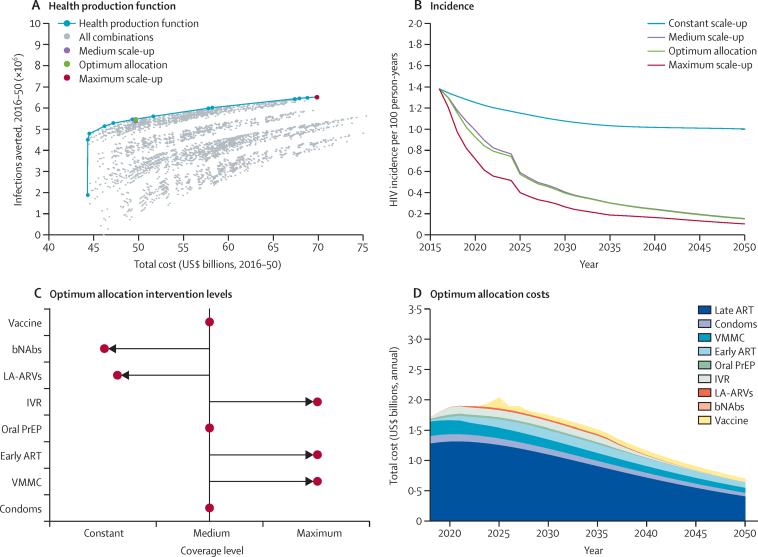
Methods: We developed a deterministic compartmental model of heterosexual HIV transmission in South Africa and formed assumptions about the costs and effects of a range of interventions, encompassing the further scale-up of existing interventions (promoting condom use, male circumcision, early antiretroviral therapy [ART] initiation for all [including increased HIV testing and counselling activities], and oral pre-exposure prophylaxis [PrEP]), the introduction of new interventions in the medium term (offering intravaginal rings, long-acting injectable antiretroviral drugs) and long term (vaccine, broadly neutralising antibodies [bNAbs]). We examined how available resources could be allocated across these interventions to achieve maximum impact, and assessed how this would be affected by the failure of the interventions to be developed or scaled up.
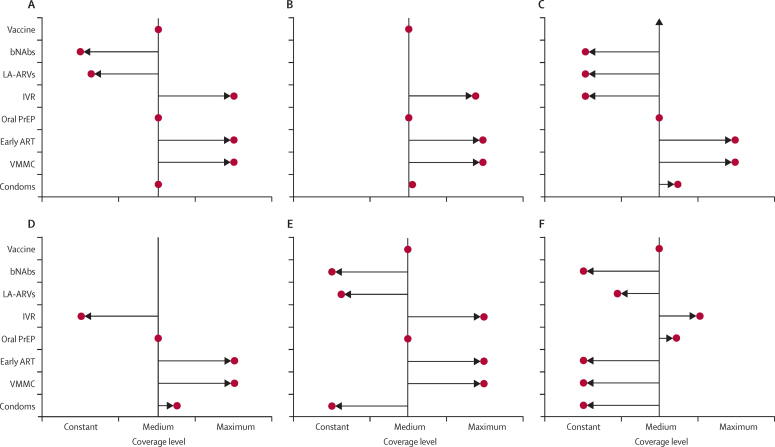
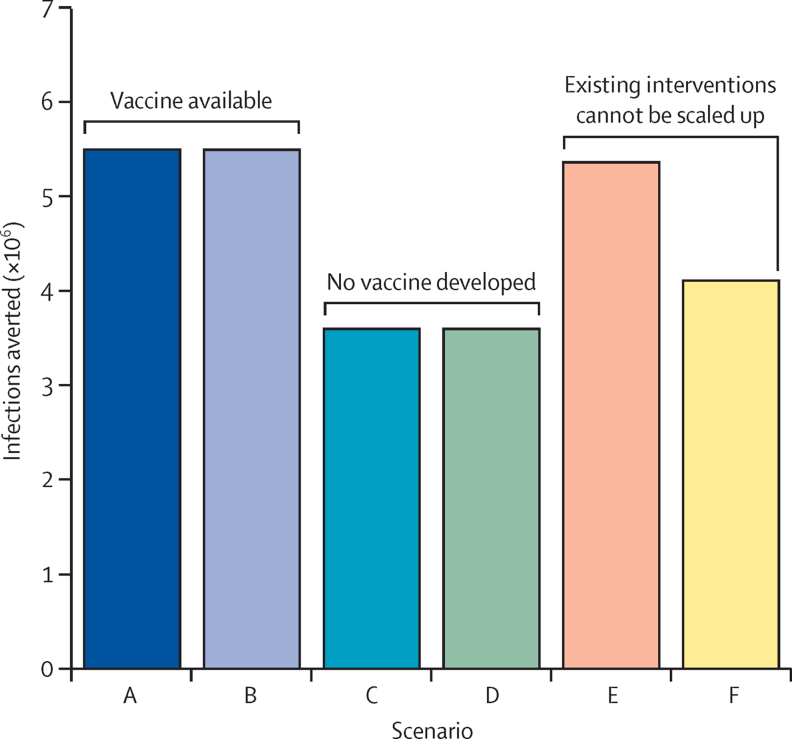
Findings: If all interventions are available, the optimum mix would place great emphasis on the following: scale-up of male circumcision and early ART initiation with outreach testing, as these are available immediately and assumed to be low cost and highly efficacious; intravaginal rings targeted to sex workers; and vaccines, as these can achieve a large effect if scaled up even if imperfectly efficacious. The optimum mix would rely less on longer term developments, such as long-acting antiretroviral drugs and bNAbs, unless the costs of these reduced. However, if impossible to scale up existing interventions to the extent assumed, emphasis on oral PrEP, intravaginal rings, and long-acting antiretroviral drugs would increase. The long-term effect on the epidemic is most affected by scale-up of existing interventions and the successful development of a vaccine.
Interpretation: With current information, a strategic approach in which limited resources are used to maximise prevention impact would focus on strengthening the scale-up of existing interventions, while pursuing a workable vaccine and developing other approaches that can be used if further scale-up of existing interventions is limited.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2016 Smith et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Legal impediments to prevention.Lancet HIV. 2016 Oct;3(10):e461. doi: 10.1016/S2352-3018(16)30157-6. Lancet HIV. 2016. PMID: 27687038 No abstract available.
References
-
- UNAIDS . On the fast-track to end AIDS by 2030: focus on location and population. UNAIDS; Geneva: 2015.
-
- Nelson KE, Celentano DD, Eiumtrakol S. Changes in sexual behavior and a decline in HIV infection among young men in Thailand. N Engl J Med. 1996;335:297–303. - PubMed
-
- UNAIDS . Fast-track: ending the AIDS epidemic by 2030. UNAIDS; Geneva: 2014.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
