

Orbital Fat Volumetry and Water Fraction Measurements Using T2-Weighted FSE-IDEAL Imaging in Patients with Thyroid-Associated Orbitopathy
- PMID: 27365323
- PMCID: PMC7963797
- DOI: 10.3174/ajnr.A4859
Orbital Fat Volumetry and Water Fraction Measurements Using T2-Weighted FSE-IDEAL Imaging in Patients with Thyroid-Associated Orbitopathy
Abstract
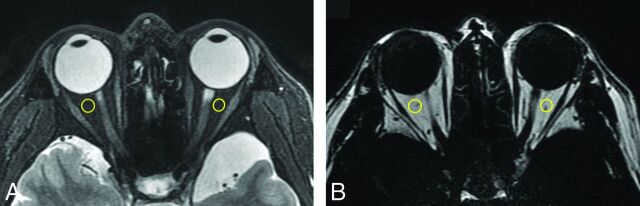
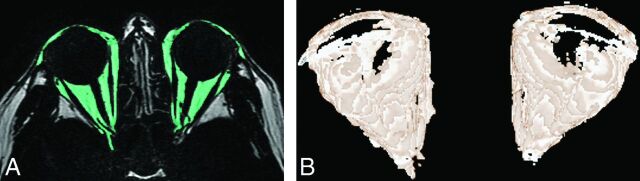
Background and purpose: The quantitative evaluation of orbital fat proliferation and edema and the assessment of extraocular muscles are useful for diagnosing and monitoring thyroid-associated orbitopathy. To evaluate therapy-induced quantitative changes in the orbital fat of patients with thyroid-associated orbitopathy, we performed volumetric and water fraction measurements by using T2-weighted FSE iterative decomposition of water and fat with echo asymmetry and least-squares estimation (FSE-IDEAL) imaging.
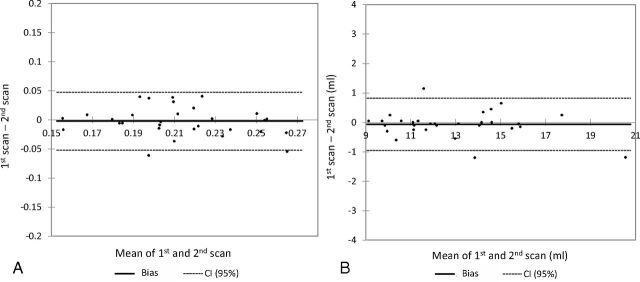
Materials and methods: Orbital FSE-IDEAL images of 30 volunteers were acquired twice within 1 week. Nine patients with thyroid-associated orbitopathy underwent FSE-IDEAL imaging before and after methylprednisolone pulse therapy, and the treatment results were assessed by using their pre- and post-methylprednisolone pulse therapy clinical activity scores. We performed volumetric and water fraction measurements of orbital fat by using FSE-IDEAL imaging and evaluated interscan differences in the volunteers. In patients with thyroid-associated orbitopathy, we compared pre- and posttherapy orbital fat measurements and assessed the correlation between the pretherapy values and clinical activity score improvement.
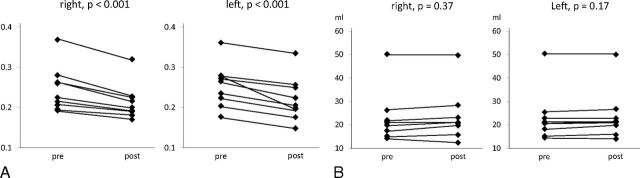
Results: The reproducibility of results obtained by the quantitative evaluation of orbital fat in volunteers was acceptable. After methylprednisolone pulse therapy, the water fraction in the orbital fat of patients with thyroid-associated orbitopathy was significantly decreased (P < .001). There was a significant positive correlation between the pretherapy water fraction and clinical activity score improvement (right, r = 0.82; left, r = 0.79) and a significant negative correlation between the pretherapy volume and clinical activity score improvement (bilateral, r = -0.84).
Conclusions: Volumetric and water fraction measurements of orbital fat by using FSE-IDEAL imaging are feasible and useful for monitoring the effects of therapy and for predicting the response of patients with thyroid-associated orbitopathy to methylprednisolone pulse therapy.
© 2016 by American Journal of Neuroradiology.
Figures
Similar articles
-
Thyroid-associated Orbitopathy: Quantitative Evaluation of the Orbital Fat Volume and Edema Using IDEAL-FSE.Eur J Radiol Open. 2019 May 18;6:182-186. doi: 10.1016/j.ejro.2019.05.003. eCollection 2019. Eur J Radiol Open. 2019. PMID: 31193388 Free PMC article.
-
Benefits and pitfalls of iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL) imaging in clinical application of the cervical spine MR.Clin Radiol. 2019 Jan;74(1):78.e13-78.e21. doi: 10.1016/j.crad.2018.09.002. Epub 2018 Oct 9. Clin Radiol. 2019. PMID: 30314808
-
Simultaneous estimation of tongue volume and fat fraction using IDEAL-FSE.J Magn Reson Imaging. 2008 Aug;28(2):504-8. doi: 10.1002/jmri.21431. J Magn Reson Imaging. 2008. PMID: 18666214 Free PMC article.
-
T1- and T2-weighted fast spin-echo imaging of the brachial plexus and cervical spine with IDEAL water-fat separation.J Magn Reson Imaging. 2006 Oct;24(4):825-32. doi: 10.1002/jmri.20721. J Magn Reson Imaging. 2006. PMID: 16969792
-
Doppler imaging of orbital vessels in the assessment of the activity and severity of thyroid-associated orbitopathy.J Ultrason. 2015 Dec;15(63):388-97. doi: 10.15557/JoU.2015.0036. Epub 2015 Dec 28. J Ultrason. 2015. PMID: 26807296 Free PMC article. Review.
Cited by
-
Radiomics analysis of the optic nerve for detecting dysthyroid optic neuropathy, based on water-fat imaging.Insights Imaging. 2022 Sep 24;13(1):154. doi: 10.1186/s13244-022-01292-7. Insights Imaging. 2022. PMID: 36153469 Free PMC article.
-
Predictive markers for anti-inflammatory treatment response in thyroid eye disease.Front Endocrinol (Lausanne). 2023 Dec 4;14:1292519. doi: 10.3389/fendo.2023.1292519. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38111706 Free PMC article. Review.
-
MRI quantitative assessment of the effects of low-carbohydrate therapy on Hashimoto's thyroiditis.Endocr Connect. 2024 Apr 22;13(5):e230477. doi: 10.1530/EC-23-0477. Print 2024 May 1. Endocr Connect. 2024. PMID: 38552311 Free PMC article.
-
Orbital fat swelling: A biomechanical theory and supporting model for spaceflight-associated neuro-ocular syndrome (SANS).Front Bioeng Biotechnol. 2023 Feb 9;11:1095948. doi: 10.3389/fbioe.2023.1095948. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 36845176 Free PMC article.
-
A Prediction Model for Detecting Dysthyroid Optic Neuropathy Based on Clinical Factors and Imaging Markers of the Optic Nerve and Cerebrospinal Fluid in the Optic Nerve Sheath.Curr Med Sci. 2024 Aug;44(4):827-832. doi: 10.1007/s11596-024-2890-2. Epub 2024 Aug 3. Curr Med Sci. 2024. PMID: 39096474
References
-
- Winand RJ, Cornet G, Etienne-Decerf J, et al. . Original acquisition in the pathogenesis and the treatment of endocrine ophthalmopathy. Metab Pediatr Syst Ophthalmol 1988;11:126–32 - PubMed
-
- Rundle FF, Wilson CW. Development and course of exophthalmos and ophthalmoplegia in Graves' disease with special reference to the effect of thyroidectomy. Clin Sci 1945;5:177–94 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources